International Journal of Pharmaceutical and Phytopharmacological Research
ISSN (Print): 2250-1029
ISSN (Online): 2249-6084

Natural products have long been used in health-related cases and have found use in contemporary folk medicine and also for developing new novel products. Firstly, because of their relative availability and safety, and lastly, for their cost-effectiveness. This study compared the wound healing potential of a formulation made from Aloe vera and honey against the use of these single agents alone. Wistar rats were grouped into 6 treatment groups. One of the animal groups received the formulation after burn wound injuries were induced to all the animals while another group received a commercially available product as the positive control. Two negative control groups were used for this study (receiving a bland gel and an untreated group) while the two remaining groups received only a single agent of Aloe vera and the other used honey. The results after the animal studies revealed that Aloe vera alone was more effective than honey or their combination for the management of wounds however antimicrobial studies that were done for these agents singly and in combination showed that honey has a better antimicrobial effect than Aloe vera. Aloe vera also helped improve the activity of honey on vancomycin and oxacillin-resistant Staphylococcus aureus (VORSA) and Escherichia coli. Aloe vera has a better wound healing potential while honey has a better antimicrobial effect. An optimal topical formulation can be made with both agents for wound healing because of their inherent synergistic antimicrobial effect on VORSA and E. coli.
INTRODUCTION
The skin is the largest organ in the human body and it’s essential for several functions, including excretion, heat management, vitamin D synthesis, protection from toxins and infections, and hydration [1, 2]. It can be affected by serious and painful wound injuries and a severe skin wound like burns can be life-threatening [2, 3]. The skin repair process includes the interaction of cells, growth factors, and cytokines in closing the lesion. The inconveniences caused by injuries, particularly chronic wounds, are mainly related to treatment and management procedures limiting wound repair, rather than tissue integrity restoration [2]. According to the World Health Organization (WHO), around 11 million people suffer from burns every year, and 180,000 die from them [3]. This is a global burden. Wound healing is also impaired in patients with diabetes which leads to foot ulcers. A recent study has shown high amputation rates from diabetic foot ulcer wounds in Nigeria and prolonged hospitalization due to poor wound healing is a source of concern [4]. Despite these alarming statistics, the investment in research support is not on par with the threat of these debilitating health issues [5]. In most cases, wounds are associated with increased morbidity as well as substantial mortality. They can extend further to other tissues and structures such as subcutaneous tissue, muscles, tendons, nerves, vessels, and bone [1].
Wounds are classified into acute and chronic. Acute wounds from unanticipated mishaps or surgical injuries typically recover in a predictable amount of time, depending on the damage's degree, size, and depth. However, over 38 million people globally suffer from chronic wounds due to flaws in the wound-healing process, which has epidemic proportions and places a significant financial burden on healthcare systems [6, 7]. The primary closure of a clean, non-serious wound requires minimal intervention to enable healing to progress naturally and quickly. Nonetheless, for chronic wounds or in a more severe traumatic injury such as a burn or gunshot wound, the presence of devitalized tissue and contamination with viable and non-viable foreign material requires surgical debridement and good antimicrobial therapy. Chronic wounds such as leg ulcers, foot ulcers, and pressure sores could be a consequence of impaired arterial or venous supply and metabolic diseases such as diabetes mellitus. They should be managed more intently and strategically [1]. Biopolymers (polymers produced by living microorganisms) are commonly used in wound management. The used materials in wound dressings involve films, sponges, fibers, or hydrogels from natural and synthetic polymers and their combinations. Ideal wound dressing should provide efficient oxygen permeability, but most importantly mimic the structural and biological characteristics of the skin's extracellular matrix [1, 8, 9]. Naturally occurring polymers from polysaccharides are generally chosen and frequently used for wound management over synthetic polymers because they are comparably economical, non-toxic to the human body, and environmentally friendly. Cellulose, chitosan, pullulan, starch, and β-glucan, as well as collagen, hyaluronic acid, and alginate are among the most used polymers as wound dressings [1]. Polymeric materials used for chronic wound dressings are reputable for their promotion of growth factors, moisture retention, enhancing neovascularization, protection from microbial agents, and tissue adhesiveness. The role of polymers in hemostasis and as a good wound-healing agent mainly depends on their biodegradability, biocompatibility, non-immunogenicity, and mechanical properties [10]. Wound dressings should be designed to facilitate and accelerate the healing process; this can be achieved by protecting the wound from factors such as contaminations and moisture loss that could delay or impair its healing [1]. These polysaccharide polymeric materials, however, do not tend to exert enough antimicrobial effects in this regard, and thus the need for supplementary therapies and research to expand the scope of wound management seems very useful. Natural polysaccharide polymers despite being more affordable to synthetic ones are still very costly and can’t be afforded by people living in low-income countries. This is where natural products like medicinal plants can come in.
Medicinal plants have been used since ancient times. It has even been estimated that nearly 80% of the world’s population relies on traditional herbal medicine for primary health care. Herbal therapies have recently shown an upward trend for a variety of ailments in parallel with the development of modern medicine. Many new drugs and treatments derived from medicinal plants are being developed and prescribed today. According to the WHO, almost 25% of modern medicines are derived from plants that were used in traditional medicine [11]. Herbs have been integral to both traditional and non-traditional forms of medicine dating back at least 5000 years. Medicinal plants, especially in wound management involve disinfection, debridement, and provision of a suitable environment for aiding the natural course of healing. Aloe vera (A. vera), just like a few other plants possesses significant wound-healing properties [12-14]. It is also known as Aloe barbadensis Miller and belongs to the family - Liliaceae. It is a typical xerophyte with thick, fleshy, strangely-cuticularized spiny leaves. It has been endorsed for a large variety of conditions and has come to play a prominent role as a contemporary folk medicine. The peeled, spineless leaves of the plant contain mucilaginous jelly from the parenchyma cells which is referred to as A. vera gel. The gel is a watery-thin, viscous, colorless liquid that contains anthraquinone glycosides, glycoprotein, gamma-linolenic acid, prostaglandins, and mucopolysaccharides that are essentially responsible for the medicinal properties including antibacterial, antifungal and its antiviral activity [12]. A. vera is widely considered an efficient herbal medicine with therapeutic uses for both diabetic and normal wounds and was reported to be more reliable and cost-effective in terms of the consistency and speed of wound healing when compared to the alternative therapies currently available [14]. Honey is another natural product that is primarily formed of glucose and fructose and is obtained from the nectar of flowers that honeybees collect. Together with other substances, it also includes vitamins, minerals, enzymes, amino acids, and organic acids [15]. Honey is very important for wound healing processes [7, 15, 16]. Natural honey has a jelly-like consistency, it forms a surface layer over wounds to prevent bacteria from entering and to keep them from drying out. Because of its high sugar content, it raises the osmotic gradient, which draws fluid up through the subdermal tissue and provides more glucose for the wound's cellular constituents to thrive [15]. The hydrogen peroxide that is produced from the glucose in honey is another characteristic that initiates antibacterial activity. Certain varieties of honey do not rely on hydrogen peroxide for their antibacterial action but possibly rely more on pH alteration and osmolarity for their bactericidal capabilities. Honey has been used for wound healing since ancient times mainly due to its antimicrobial activity. In addition to the broad spectrum of antibacterial activity against common wound-infecting microorganisms, honey has been demonstrated to be effective against antibiotic-resistant bacteria and was able to restore the efficacy of some antibiotics against bacteria with previously acquired resistance [7, 15]. Some studies have been done involving both A. vera and honey formulated as a gel for wound healing [17-19], but there has not been an extensive in vivo study that reveals the comparison of effects of its combination to the single use of A. vera or honey.
This research aims to formulate and evaluate the comparative wound healing potentials of a formulation made from A. vera and honey gel against the use of the two agents singly for the management of skin burns.
MATERIALS AND METHODS
Materials
A. vera plant (sourced from Awka, Nigeria), pure honey (sourced from Enugu, Nigeria), methylparaben (Lobechem, India), propylparaben (Lobechem, India), Mueller-Hinton Agar ‘MHA’ (Oxoid Limited, England), ascorbic acid (Lobechem, India), glycerine (Lobechem, India), carboxy methyl cellulose (Griffin and George, India), Silver sulfadiazine cream ‘Dermazine®’(purchased from Awka, Nigeria), cotton wool (purchased from Onitsha, Nigeria), ketamine hydrochloride ‘Ketalar®’ (purchased from Onitsha, Nigeria), shaving cream ‘Veet®’ (purchased from Awka, Nigeria), etc.
Methodology
Extraction of A. vera gel
The plant after being sourced, was authenticated by a botanist and deposited in the herbarium of the Department of Pharmacognosy and Traditional Medicine, Faculty of Pharmaceutical Sciences, Nnamdi Azikiwe University, Agulu, Anambra State, Nigeria with the voucher number of the plant obtained - PCG/504/L/033. The gel from the plant was extracted per the method of Uddin et al. [20] with slight modifications. The leaves were cleaned with distilled water. The extraction of A. vera gel was performed by making an incision on the parenchymatous covering of the leaves. The gel was then put in a suitable container and stored in a refrigerator at 5 ºC for further use.
Sourcing and storage of honey
Pure honey was sourced commercially from a certified supplier, and stored in a refrigerator at 5 ºC for further use.
Culture media and reagents
The culture media used were nutrient broth and MHA. The culture media were prepared according to the instructions of the manufacturers. The manufacturers specify that the media should be prepared by dissolving 38 grams of MHA in enough distilled water or deionized water to make one liter of solution sterilized by autoclaving at 15 psi at 121 °C for 15 min. After autoclaving it was left to cool to 50 °C and was poured immediately into a flat bottom petri dish on a horizontal surface. Reagents used include Mc Farland 0.5 turbidity standard (prepared from barium chloride, sulfuric acid, and water), and sodium hypochlorite solution.
Test organisms used
Vancomycin and oxacillin-resistant Staphylococcus aureus (VORSA) and sensitive strains of Pseudomonas aeruginosa, Staphylococcus aureus, and Escherichia coli were used and are all clinical isolates obtained from the Department of Pharmaceutical Microbiology and Biotechnology, Nnamdi Azikiwe University, Awka, Nigeria.
Preliminary antimicrobial evaluation: biochemical test for the confirmation of the resistant Staphylococcus aureus
Determination of in vitro antimicrobial activity of A. vera and honey extracts
The antibacterial activity of the A. vera and honey extracts was evaluated by the cup plate agar diffusion method as described by Massoud et al. [23] with slight modification. The microorganisms used in this test were the human pathogenic bacteria VORSA and the sensitive strains of P. aeruginosa, S. aureus, and E. coli. The bacterial cultures were adjusted to 0.5 McFarland turbidity standard then each of the test organisms was swabbed on the surface of sterile MHA (diameter: 90 mm). A sterile cork borer was used to make wells (8 mm in diameter) on each of the MHA. Graded concentrations of the A. vera and honey samples were made using sterile distilled water as the diluent. 100, 50, 25, 12.5, 6.25, and 3.125 mg/ml of A. vera gel and honey were prepared with appropriate volumes of sterile distilled water. 80 µl of the different dilutions were applied into their respective well in the agar plate already seeded with the test organisms. The cultures were incubated at 37 °C for 24 hours. Antimicrobial activity was determined by measuring the zone of inhibition (ZOI) around each well (excluding the diameter of the well). For each concentration, three replicate trials were conducted against the test organisms.
In vitro antimicrobial synergistic study
The determination of the synergistic antibacterial activity of the combination of A. vera and honey was done using the same antimicrobial procedure as described above. The A. vera and honey mixtures were prepared in the ratios of 5:0, 4:1, 3:2, 2:3, 1:4, and 0:5 by volume (v/v) respectively. Here, separate solutions of the two agents were prepared with the diluent and thereafter, the solutions were combined in these different ratios, preferably, adopting the continuous variations model. An aliquot of 80 µL of each of the combinations was applied into their respective well in the agar plate already seeded with the test organisms. The plates were then incubated at 37 °C for 24 hours. Antimicrobial activity was determined by measuring the ZOI around each well (excluding the diameter of the well). For each concentration, three replicate trials were also conducted against the test organisms.
Preparation of bland gel
Table 1. Formula and constituents of the bland gel
|
Ingredient |
Percentage (%) |
|
Carboxymethylcellulose |
3.0 |
|
Methylparaben |
0.2 |
|
Propylparaben |
0.1 |
|
Glycerine |
10.0 |
|
Ascorbic acid |
0.1 |
|
Water |
qs to 100 % |
100 g quantities were prepared and excipients were combined as shown (Table 1). The methylparaben (0.2 g), propylparaben (0.1 g), and ascorbic acid (0.1 g) were dispersed in about 50 ml of water. To this, 10 ml of glycerine was added and the mixture was stirred using a homogenizer (Jingxin F013200021 China), set at 10000 rpm for 10 minutes. Carboxymethylcellulose (3 g) was then gently dispersed in the mixture and stirring continued for about 10 minutes until the gelling agent had been completely dispersed. Water was then used to make up to 100 ml volume with a further 3 minutes of homogenization. The mixture was then left overnight for complete hydration and stored at room temperature (28 °C) until when needed.
Formulation of gel using an optimized combination of A. vera and honey
Table 2. Formula and constituents of the formulated gel containing A. vera and honey
|
Ingredient |
Quantity (ml) |
Percentage (%) |
|
A. vera gel |
2 |
10 |
|
Honey |
8 |
40 |
|
Bland gel |
10 |
50 |
The A. vera-honey combination ratio with the best activity from the microbiological synergistic study was used to represent 50% of the formulation while the bland gel represented the other 50% (Table 2). Using a 25 ml measuring cylinder; 2 ml of A. vera gel, 8 ml of honey, and 10 ml of bland gel (50%) were all measured out and carefully transferred into a beaker. Using a homogenizer (Jingxin F013200021 China), set at 10000 rpm for 20 minutes, a fully homogenous formulation was obtained. The formulation was transferred into a suitable container and stored at 5 °C for further use.
In vivo, an animal study using Wistar rats
24 healthy male and non-pregnant female Wistar rats weighing between 250 and 300 g were used. The rats were kept in separate cages and acclimatized at laboratory room temperature in Nigeria at 33 ± 2 ºC for one week before they were used. They had unrestricted access to drinking water and food. Also, proper light and dark cycles were observed. The animals were first anesthetized using the method described by Yassine et al. [24] with slight modifications. Ketamine hydrochloride (100 mg/kg) was administered to the animals intraperitoneally on day 0. Dorsum hairs were removed using a commercially available ointment (Veet®) and a dissecting set before administering the anesthetic agent (ketamine hydrochloride). Subsequently, second-degree burn injury was induced using the rat scald burn model as described by [25]. The burn areas were exposed to boiling water for 10 seconds after which they were removed. The animals were then placed in six groups of four animals each. The diameter of the burn area was noted and administration of the preparations commenced on day 1.
Group 1 animals were treated using the bland gel. Group 2 animals were treated using A. vera gel alone. Group 3 animals were treated using honey alone. Group 4 animals were treated using the A. vera made with the optimized combination of A. vera and honey obtained from microbiological studies. Group 5 served as the positive control treated with a commercial preparation of silver sulphadiazine cream (Dermazine®) while group 6 was left untreated. About 0.5 g of the preparations were used to treat the animals once daily while wound diameter was assessed every three days. Treatment lasted for 21 days. The time of acquiring complete epithelialization was considered as the time of wound healing progression. Also, the skin color changes in the burn area as well as the presence of inflammation in the burn areas were observed. Percentage wound contraction was determined using the Eq. 1.
|
|
(1) |
The wound area images were also used for visual comparison.
RESULTS AND DISCUSSION
Biochemical test result for identification and confirmation of S. aureus
Effervescence (positive result) was observed for the catalase test. Effervescence during a catalase test refers to the production of bubbles which indicates the release of oxygen gas which confirms the presence of catalase, meaning the bacteria in the sample is likely from the Staphylococcus genus [21]. A negative result (no color change) showed for the oxidase test also confirmed the identification of S. aureus as it is oxidase-negative [22].
This preliminary antimicrobial investigation was done for only S. aureus as it’s a resistant strain while the other test organisms are sensitive strains.
In vitro antimicrobial activity of A. vera and honey extracts
Table 3. Result of the antimicrobial evaluation of A. vera against the test organisms
|
Test organisms |
Concentration v/v (%) / Zone of inhibition (mm) |
|||||
|
100 |
50 |
25 |
12.5 |
6.25 |
3.13 |
|
|
VORSA |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
|
S. aureus (sensitive) |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
|
P. aeruginosa (sensitive) |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
|
E. coli (sensitive) |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
Note. VORSA: Vancomycin and Oxacillin-Resistant S. aureus
Table 4. Result of the antimicrobial evaluation of honey against the test organisms
|
Test organisms |
Concentration v/v (%) / Zone of Inhibition (mm) |
|||||
|
100 |
50 |
25 |
12.5 |
6.25 |
3.13 |
|
|
VORSA |
5 ± 0.7 |
2 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
|
S. aureus (sensitive) |
13.3 ± 0.6 |
11 ± 1 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
|
P. aeruginosa (sensitive) |
15 ± 1 |
11.3 ± 1.2 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
|
E. coli (sensitive) |
8 ± 0 |
3 ± 0.7 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
Note. VORSA: Vancomycin and oxacillin-resistant S. aureus
From the microbiological evaluation carried out on A. vera and honey, the former showed no activity against the test organisms (Table 3) but the latter showed activity against all – VORSA, sensitive S. aureus, P. aeruginosa, and E. coli (Table 4). From the experimental results obtained, it can be said that honey exhibits antibacterial activity against some organisms implicated in delayed wound healing, specifically the test organisms, while A. vera does not. Based on this, it can be confirmed that the role/ effect of honey in wound healing mechanism is attributed to its antimicrobial activity as alluded to in the literature [7, 15, 16]. This is due to its enzymatic production of hydrogen peroxide and its low pH level and high sugar content (high osmolarity) which is enough to hinder the growth of microbes. This further explains the reason for its activity at high concentrations with a minimum inhibitory concentration (MIC) of 50%. Honey is also postulated to bring about wound healing through its chemical debridement and anti-inflammatory activity [26]. The inability of A. vera to exert any antimicrobial effect on the test organisms can be a result of the plant species' biotic/abiotic environment, growth conditions, and other phytochemical and environmental factors involved in plant growth and activity. It has been stated that the physicochemical properties of A. vera are highly dependent on the species, climate, region, growing conditions, processing, and storage methods, which can result in important changes in terms of both chemical constituents and therapeutic properties [27]. Improving the standardization and the quality control assessment of A. vera products may help avoid this variability [28].
In vitro antimicrobial synergistic study
Table 5. Result showing the zone of inhibition of the various combinations of A. vera and honey
|
Combination ratio A. vera: Honey |
Zone of inhibition (mm) |
|||
|
VORSA |
S. aureus |
E. coli |
P. aeruginosa |
|
|
5:0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
0 ± 0 |
|
4:1 |
0 ± 0 |
6.7 ± 0.6 |
0 ± 0 |
0 ± 0 |
|
3:2 |
0 ± 0 |
5 ± 0 |
0 ± 0 |
2 ± 0 |
|
2:3 |
0 ± 0 |
0 ± 0 |
4.3 ± 0.6 |
0 ± 0 |
|
1:4 |
5.7 ± 1.53 |
2 ± 0 |
5 ± 1 |
2.7 ± 0.6 |
|
0:5 |
4.3 ± 0.6 |
4.7 ± 0.6 |
4.3 ± 0.6 |
5 ± 0 |
An in vitro antimicrobial study was carried out to investigate the effect of the combination of A. vera and honey (possible synergism) and to thus inform the most optimal combination ratio to be used for the gel formulation (Table 5). The combination of A. vera and honey showed good antimicrobial activity at ratios of 1:4 and 0:5, respectively. No antimicrobial activity was detected for the ratio of 5:0 for all the test organisms. This result showed that honey alone was capable of inhibiting all the test organisms and A. vera alone can’t inhibit all the test organisms but of great reveal from this experiment is that A. vera however helps improve the action of the mix synergistically as shown with the 1:4 combination ratio especially for the VORSA and E. coli test organisms alone, (IZD of 5.7 ± 1.53 mm and 5 ± 1 mm, respectively). The 1:4 (A. vera: honey) combination ratio was more effective on the resistant strain of the organism (VORSA) and as such was chosen as the optimal combination ratio for the formulation.
In vivo animal study
|
|
|
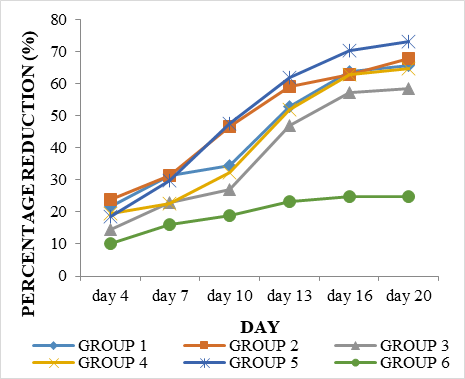
Figure 1. Graphical representation of percentage reduction of wound over time for the different treatment groups |
Table 6. Period of wound epithelialization for all the treatment groups
|
Groups |
Treatment |
Perıod of wound epithelialization |
|
1 |
Bland gel |
Day 15 |
|
2 |
AV gel alone |
Day 10 |
|
3 |
H alone |
Day 13 |
|
4 |
AV: H gel formulation |
Day 13 |
|
5 |
SSD cream (positive control) |
Day 13 |
|
6 |
Untreated |
DAY 18 |
Note. AV- A. vera; H- Honey; SSD- Silver sulfadiazine
The progression of the healing process accessed at every 3–day interval was measured for all the treatment groups (Figure 1). It showed results of faster onset of action with the positive control cream (though not up to full epithelialization) whilst also showing good activities for the A. vera gel alone, honey alone, and the formulation. The period of wound epithelialization is calculated as the number of days required for the scar to completely fall off, leaving no raw wound [29]. Epithelialization varied for different groups and was reached at day 10 for group 2 administered A. vera gel alone while groups 3, 4, and 5 animals administered the honey alone, formulation and the positive control cream respectively achieved the same feat on day 13 (Table 6). Epithelialization is an essential component of wound healing and is used as a defining parameter of its success. In the absence of re-epithelialization, a wound cannot be considered healed [29, 30]. The bland gel showed an epithelialization time of 15 days and the untreated group showed an epithelialization time of 18 days. This result implies that groups presenting a shorter period of epithelialization of the wounded area will produce a faster healing that results in regeneration but for the groups with a slower period of epithelialization, a scar will form for a longer time. Timing is important to wound healing. Critically the timing of wound epithelialization can decide the outcome of healing. If the epithelialization of tissue over a denuded area is slow, a scar will form over many weeks or months but if the epithelialization of the wounded area is fast, the healing will result in regeneration faster [29, 31].
Upon infliction of a wound, inflammation was observed, animals expressed extreme pain, the wound area was clearly defined and even coloration of skin was observed. After the 21-day treatment, the treatment groups 1 to 5 completely healed, wound contraction was greatly visible, and complete wound epithelialization had occurred. The sequence of events that repairs the damage is categorized into four overlapping phases: hemostasis, inflammation, proliferation, and tissue remodeling. The final step of the proliferative phase is the epithelialization [32]. Several studies showed that burn infection is the major cause of mortality in patients with extensive burns, therefore many researchers tried to achieve appropriate treatment methods to reduce the risk of wound infections and shorten the period of treatment by enhancing tissue repair, skin regeneration, and epithelialization [33-35].
From this research study, it can be inferred that the major role of honey in wound healing is attributed to its ability to inhibit microbial growth, hence fastening the healing process. Also, judging from the result of the antimicrobial analysis, where A. vera had no effect, and the result of the animal studies where it played a significant role, it can be inferred that the healing potential of A. vera can be majorly attributed to the inhibition of pain and inflammation; stimulation of fibroblast to functionally increase collagen and proteoglycans; wound contraction and epithelialization. In a recent study, it has been revealed that the key regulator of the action of A. vera in promoting healing is the existence of a mannose-rich polysaccharide; called glucomannan which acts together with gibberellin and growth hormone stimulating fibroblasts to proliferate actively [14]. Upon triggering fibroblast activation and proliferation, collagen biogenesis significantly increases both quantitatively and qualitatively. They also stated that it accelerates wound healing not only through promoting the active proliferation of fibroblasts but also because it shows protective action for keratinocytes.
CONCLUSION
The findings of this study collectively suggest that A. vera gel alone has a better wound-healing property on the animal subjects than honey while honey proved to have a better antimicrobial property than A. vera gel. This emphasizes the need for the combination of both plants for an optimum effect, as the combination of A. vera and honey was also synergistically effective against Vancomycin and Oxacillin-resistant strains of Staphylococcus aureus.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: Animal experiments were conducted after obtaining ethical approval from the animal research ethics committee of Nnamdi Azikiwe University, Awka, Nigeria with approval number NAU/AREC/2013/0025.