International Journal of Pharmaceutical and Phytopharmacological Research
ISSN (Print): 2250-1029
ISSN (Online): 2249-6084

Glucagon-like peptide-1 (GLP-1) overpowers glucagon secretion, endorses satiety, postpones gastric draining, and arouses peripheral glucose consumption. This systematic review was carried out including PubMed, Google Scholar, and EBSCO that examined randomized controlled trials, observational, and experimental studies that had studied the role of GLP-1 (liraglutide) in controlling juvenile diabetes. The study included 7 studies and concluded that the introduction of liraglutide to insulin treatment juvenile diabetic patients results in a considerable and fast decrease in glycemic excursions and a consequent reduction in insulin dose. Body weight decreases substantially as reported in many studies.
INTRODUCTION
Glucagon-like peptide 1 (GLP-1) receptor agonists are an effective add-on therapy choice to achieve reduced insulin doses, weight loss, and moderate increases in hemoglobin A1c (HbA1c) levels without dramatically raising the risk of hypoglycemia [1]. GLP-1 is an incretin hormone released from enteroendocrine L cells to respond to ingested nutrition. The management of juvenile diabetes is dynamic and has many difficulties. Enhancement of glycemic control serves a significant role in the preclusion of both macro and microvascular complications but also results in undesired weight gain and adverse health outcomes [2].
Hyperglycemia in type 1 diabetes is demonstrated by a "bi-hormonal" malfunction, as both losses of insulin and excessive glucagon lead to higher glucose levels [3, 4]. Throughout, it’s been found that in people with type 1 diabetes, loss of glucagon inhibition after a meal leads to postprandial hyperglycemia [5, 6]. In addition, the glucagon reaction to hypoglycemia is insufficient or missing, which may contribute to serious hypoglycemia during insulin therapy [7]. During hypoglycemia, people with T1D rely on the consumption of quick-acting carbohydrates, the accelerated GE pace, and the reaction of regulatory hormones to recover from the crisis. Glucagon reactions are gradually neutralized with long-standing T1D and any more disruption of glucagon and other counter-regulatory hormone reactions during therapy with GLP-1RA raises the risk of serious hypoglycemia [8].
The first known and perhaps most important function of GLP-1 is the potentiation of glucose-stimulated insulin secretion in beta cells, regulated by the stimulation of its seven G-protein-coupled transmembrane domain receptors. In parallel to its insulin-tropical function, GLP-1 exerts an islet-trophic effect by promoting proliferation and differentiation and by minimizing beta-cell apoptosis. GLP-1 suppresses glucagon secretion, endorses satiety, postponements gastric draining, and arouses peripheral glucose consumption [9].
MATERIALS AND METHODS
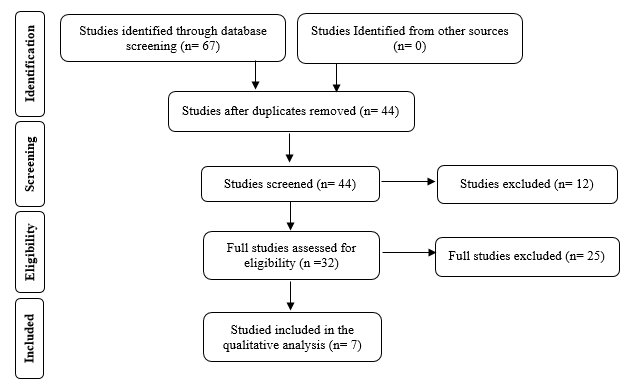
PubMed and EBSCO Information Services were chosen as the search databases for the publications used within the study, as they are high-quality sources. liraglutide in the management of type 1 diabetes mellitus and other articles have been helped us in the creation of the article. Restriction to the last 10 years and English language due to unavailable resources for translation were used [10-13]. The originated papers were sorted by titles, and rereading the summaries yielded 7 articles that were enrolled (Figure 1). Inclusion criteria: the articles were selected based on the relevance to the project, which should include one of the following topics; ‘liraglutide, T1DM, management of diabetes mellitus, GLP-1’. Exclusion criteria: all other articles that did not have one of these topics as their primary end, or repeated studies, and reviews studies have been excluded.
Statistical analysis
The data was extracted based on a specific form that contained (Title of the publication, author’s name, objective, summary, results, and outcomes). These data were reviewed by the group members to determine the initial findings and the modalities of performing the surgical procedure. Double revision of each member’s outcomes was applied to ensure the validity and minimize the mistakes.
RESULTS AND DISCUSSION
The search of the mentioned databases returned a total of 67 studies that were included for title screening. 44 of them were included for abstract screening, which led to the exclusion of 12 articles. The remaining 32 publications’ full-texts were reviewed. The full-text revision led to the exclusion of 25 studies, and 7 were enrolled for final data extraction (Table 1) [14, 15].
|
|
|
Figure 1. Flow chart illustrating the process of data extraction |
Table 1. Author, year of publication, study type, and study outcome
|
Author Study Region Year of publication |
Study type |
Sample size |
Outcome |
|
Frandsen, CS et al. [16] Denmark 2016 |
randomized, double-blinded, placebo-controlled study |
20 patients |
Liraglutide does not affect glycemic recovery, GE intensity or counter regulatory hormone response in T1D during hypoglycemia. |
|
MathieuC, et al. [17] 17 countries 2016 |
Randomized Trial |
1,398 adults |
Liraglutide supplementary to insulin treatment decreases HbA1c levels, insulin dosage, and body weight in people who are mostly representative of individuals who had juvenile diabetes, characterized by higher rates of symptomatic hypoglycemia and hyperglycemia with ketosis, thus restraining clinical use in those individuals |
|
Kuhadiya N. D, et al. [18] Western New York 2016 |
Randomized Placebo-Controlled Clinical Trial of 12 Weeks |
72 patients |
Adding 1.2 mg and 1.8 mg liraglutide to insulin in a period of above 3-months in overweight and obese cases with juvenile diabetes leads to the modest decrease of the mean glucose levels by substantial weight reduction, low insulin dosage decreases, and common gastrointestinal complications. These conclusions do not validate using of liraglutide in wholly cases of juvenile diabetes. |
|
Frandsen, Christian S et al. [19] Denmark 2015 |
A Randomized, Placebo-Controlled, Double-Blind Parallel Study |
40 patients |
Liraglutide significantly reduces body weight and insulin requirements but has no additional effect on HbA1c in normal-weight patients with type 1 diabetes inadequately controlled on insulin alone. |
|
Ahr ́en B, et al. [20] 59 centers in North America, Europe, and Africa 2016 |
The ADJUNCT TWO Randomized Trial |
835 subjects |
In a large sample of cases with long-lasting juvenile diabetes, the addition of liraglutide to topped insulin abridged HbA1c, body weight, and insulin supplies nevertheless with increased frequency of hypoglycemia for liraglutide 1.2 mg & hyperglycemia with ketosis for liraglutide 1.8 mg. |
|
Dejgaard, Thomas Fremming et al. [21] Denmark 2015 |
randomized, double-blind, placebo-controlled trial |
100 patients |
Liraglutide remained linked with drops in hypoglycemic proceedings, bolus and whole insulin amount, bodyweight, and raised pulse rate. |
|
Janzen, Kristin M et al. [22] ---- 2016 |
Review Article |
9 clinical trials |
GLP-1 agonists must be used in overweight or obese juvenile DM cases that are not at glycemic goals in spite of hostile insulin therapy; though, acceptability of these means is a probable distress. Liraglutide possess the strongest proof for use and it is the best choice in overweight or obese adult cases with uncontrolled juvenile DM. |
A recent 52-week trial showed no improvement in the frequency of hypoglycemia [23]. In a systematic study and meta-analysis performed by Dimitrios, Patoulias, et al. [24], 5 experiments of 2,445 randomized participants recorded better glycemic regulation and recovery of hypoglycemia. A significant increase in heart rate was also observed as reported by Dejgaard, Thomas Fremming et al. [21]. This agreed with Varanasi, Ajay et al. [25] who reported that liraglutide improved glycemic control in type 1 diabetes (HbA1c decreased significantly at 24 weeks from 6.5 to 6.1% (P=0.02)) and DANDONA P, et al. [26] in a 52-week randomized double-blinded placebo-controlled clinical trial also reported significantly reduced HbA1c but increase in hypoglycemia.
The loss of weight and subsequent suppression of appetite, also for a brief duration of therapy, are of concern. Liraglutide is known to have an appetite suppressive effect. This effect of liraglutide is significant because 40–50 percent of patients with type 1 diabetes across the US have metabolic syndrome [27]. After all, weight loss was not sufficient to decrease the insulin dosage as it happened within the first 2 days of initiation of liraglutide treatment. The reduction of body weight has consequences for cardiovascular risks [28]. Significant weight loss after liraglutide use was reported by Mathieu C, et al. [17], Kuhadiya N. D, et al. [18], Frandsen, Christian S et al. [19], Ahr ́en B, et al. [20], Dejgaard, Thomas Fremming et al. [21] and Janzen, Kristin M et al. [22]. Similar reports were found in many other studies [24-26].
While patients with long-standing type 1 diabetes do not have substantial insulin secretion, it has been seen that they have a significant β-cell population that is not totally segregated. Long-term treatment can likely promote the complete differentiation of these cells and restore some insulin secretion [29]. Decreasing exogenous insulin requirements were reported by Dimitrios, Patoulias et al. [24] agreeing with Dejgaard, Thomas Fremming et al. [21], and MathieuC, et al. [17]. Varanasi, Ajay et al. [25] also reported that basal and bolus insulin doses also significantly decreased (P<0.01). In contrast, Dandona P, et al. [26] reported no alteration in total insulin dose. Rother et al. [30] showed an improvement in insulin secretion over a span of several months, but this was not found clinically significant.
CONCLUSION
The introduction of liraglutide to insulin therapy in type 1 diabetics results in a considerable and fast decrease in glycemic excursions and a consequent reduction in insulin dose. Body weight decreases substantially as has been reported in many studies. Cardiovascular events may be associated.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None