International Journal of Pharmaceutical and Phytopharmacological Research
ISSN (Print): 2250-1029
ISSN (Online): 2249-6084

Blood glucose control is challenging in hemodialysis (HD) patients. In this study, we aimed to characterize blood glucose fluctuations during HD in end-stage renal disease patients and predict risk factors for hypoglycemia. A cross-sectional study was performed including all adult patients receiving hemodialysis at a tertiary care hospital. Each patient was evaluated through three HD sessions. Descriptive analysis of all the demographic and outcomes variables was performed to establish blood glucose patterns during HD and hypoglycemic events during HD sessions.
We had a total of 20 patients, with a total of 60 HD sessions. The patients’ mean age was 45 years, and the mean duration since the initiation of HD was seven years. The mean blood sugar levels at pre-, mid-, and post-dialysis were 7.9 mmol/dl (CI 7.3-8.6), 6.4 mmol/dl (CI 5.9-6.9), and 5.9 mmol/dl (CI 5.4-6.3), respectively. There were six episodes of hypoglycemia, and all episodes except for one occurred in patients without a history of diabetes. None of the variables were found to have a statistically significant association with the development of hypoglycemia. There was a clear downward trend in blood glucose during the course of HD.
INTRODUCTION
Chronic kidney disease (CKD) is defined by kidney damage or impairment in kidney function for three or more months irrespective of the cause [1-3]. End-stage renal disease (ESRD) is the late stage of CKD that requires renal replacement therapy by either hemodialysis (HD) or peritoneal dialysis (PD) in ambulatory patients [4, 5]. In Saudi Arabia, the prevalence of ESRD is estimated to be 604 cases per million population as per the Saudi Center for Organ Transplantation [6].
Well-established risk factors for CKD and ESRD are advanced age, hypertension, and diabetes mellitus (DM), which has become the leading cause of ESRD in recent decades [7].
Blood sugar control is challenging in ESRD patients. Those patients are more prone to develop hypoglycemia secondary to decreased insulin degradation, as well as due to malnutrition, impaired gluconeogenesis, and dialysate solution in HD\PD affects insulin clearance [8, 9]. Thus, patients with DM are at increased risk of developing wide fluctuations in blood glucose during HD and also between the dialysis days and off-dialysis days [10], and thus blood glucose monitoring during HD is often necessary. Whether the same concept applies to patients without DM is scarcely studied.
In this study, we aimed to characterize the pattern of blood glucose variability during HD in patients with and without DM. We also aimed to identify factors predicting the development of hypoglycemia during HD in patients with ESRD.
MATERIALS AND METHODS
Patients
We included patients with ESRD receiving HD regularly in the outpatient HD unit. Patients who were 14 years of age or older with and without type 1 or 2 DM were included. We excluded clinically unstable patients, patients with ongoing systemic infections, or hospitalized for a concurrent illness. Patients who were taking steroids, or medications affecting blood sugar readings apart from DM control medications were also excluded, and patients who declined participation in the study.
Written informed consent was secured from all participating patients, and the institutional review board approved the study.
Study design
We conducted a cross-sectional study at the HD unit at a tertiary care center over a period of one month.
Patients’ data collected include age, sex, dry weight, DM status, and duration if applicable. Also, we documented the prescribed antidiabetic medication, the time since HD was initiated, and the length of HD sessions. The albumin was chosen to reflect the patients' nutritional status and Erythrocyte Sedimentation Rate (ESR) as an inflammatory marker.
Each patient was evaluated through three HD sessions. Glucose readings were measured pre-, mid-, and post HD sessions. Glucose samples were collected from the arterial line of the HD system and measured by a glucometer. Patients were instructed to fast only during the HD session. The time of the last meal or snack was also recorded. Hypoglycemia was defined by either biochemical hypoglycemia where blood glucose is less than 70 mg/dl or 3.8 mmol/L.
Statistical analysis
Descriptive analysis of all the demographic and outcomes variables was performed. Data analysis was performed by using Stata SE version 16.1 (StataCorp LLC, TX). The main outcome of this study was blood sugar patterns during HD and hypoglycemic events during HD sessions. We incorporated all variables in a univariate and multivariate analysis to establish the odds ratio for each variable. We used a modified logistic regression. Variables with a p-value of more than 0.2 were excluded from the final analysis.
RESULTS AND DISCUSSION
We had a total of 20 patients after applying the inclusion and exclusion criteria, with a total of 60 analyzed HD sessions. All the HD sessions utilized glucose-free dialysate. The mean age was 45 years, and the mean duration since the initiation of HD was seven years. Most of the patients were females (55%) and not known with DM (75%). Only one patient with DM was on long-acting insulin, and the rest were between diet and oral hypoglycemic medications (OHM). Table 1 demonstrates the demographic and baseline characteristics of the study patients.
Table 1. Demographic and baseline characteristics of the study patients
|
Variable |
Mean (SD) N (%) |
|
Age |
45.1(37.1-52.0) |
|
Gender Male Female |
9 (45%) 11 (55%) |
|
Mean dry weight (Kg) |
60.3 (6.1-6.7) |
|
Diabetes type Type 1 Type 2 None |
0 (0%) 5 (25%) 15 (75%) |
|
Duration of diabetes (years) |
7.0 (4.6-9.4) |
|
Duration of HD (hours) |
1.17 (1.03-1.29) |
|
Serum albumin |
30.0a (27.2-32.7) |
|
CRPb |
10.6 (5.3-15.2) |
|
WBC |
6.4x109(5.5-7.3) |
|
Diabetes treatment Insulin OHMc NA |
1 (5%) 4 (20%) 15 (75%) |
a Albumin is g/L, bC-reactive protein.
cOral hypoglycemic medications
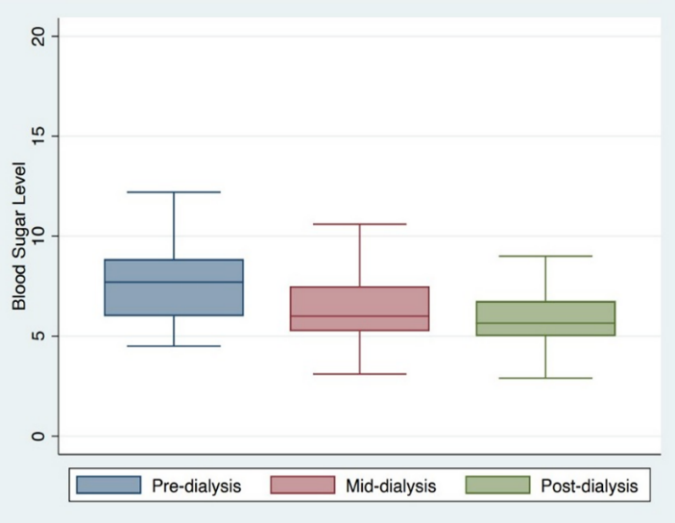
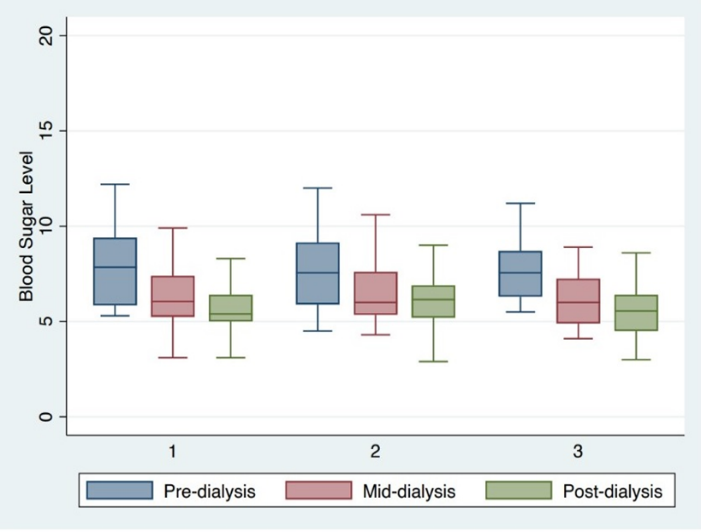
There was a clear trend toward a reduction in the mean blood sugar level during the course of HD sessions. The mean blood sugar levels at pre-, mid-, and post-dialysis were 7.9 mmol/dl (CI 7.3-8.6), 6.4 mmol/dl (CI 5.9-6.9), and 5.9 mmol/dl (CI 5.4-6.3), respectively. None of the HD sessions were interrupted or paused, even those that had an episode of hypoglycemia. Figure 1 illustrates the mean blood sugar level of the participating patients at all stages of HD, and Figure 2 illustrates the mean blood sugar level of the participants per each HD session. The mean difference in blood glucose levels between the pre- and post-dialysis levels was 2.04 mmol/dl (CI 1.5-2.6).
|
|
|
Figure 1. Mean blood sugar of the participating patients at all stages of HD |
|
|
|
Figure 2. Mean blood sugar of the participants per each HD session |
There were six episodes of hypoglycemia among 6 study participants, representing an incidence of 10% of the whole sessions, with blood sugar ranging between 2.9-3.7 mmol/dl. All hypoglycemic episodes occurred in patients who had pre-dialysis blood glucose levels equal to or below the mean pre-dialysis blood glucose (7.9 mmol/dl) at a range between 4.5-7.9 mmol/dl. All episodes except for one occurred in patients without a history of DM. In non-diabetic patients, the hypoglycemic episodes were asymptomatic. However, diabetic patients have experienced sweating and drowsiness.
All hypoglycemic episodes except for one occurred at the end of the HD session. Only one episode occurred at mid-dialysis in a patient without DM, and the reading was 3.1 mmol/dl. The other five hypoglycemic episodes were at the post-dialysis period. Four of these episodes were in patients without DM and one in a patient with a history of OHM-treated DM. This patient received his OHM 14 hours before the HD session, and the blood sugar at the time of hypoglycemia was 3.7 mmol/dl, and the patient was symptomatic for hypoglycemia. Patients who developed hypoglycemia were treated with either a snack or 50ml of intravenous D50 dextrose solution, whether symptomatic or not.
We applied multivariate analysis to study the association between HD-related hypoglycemia and the following variables; age, duration of HD since the first session, the period from the last meal or snack till HD time. None of these variables were found to have a statistically significant association with the development of hypoglycemia (Table 2).
Table 2. Univariate and Multivariate analysis of the association between hypoglycemia and clinical characteristics
|
|
Univariate Analysis |
Multivariate Analysis |
||||
|
Variable |
OR |
95% C.I |
P-value |
OR |
95% C.I |
p-value |
|
Age |
0.90 |
0.9-1.0 |
0.30 |
0.85 |
0.55-1.32 |
0.47 |
|
Duration of HD(years) |
0.99 |
0.88-1.12 |
0.94 |
1.56 |
0.48-5.02 |
0.46 |
|
Last meal/snack prior to HD (hr) |
1.195 |
.92-1.6 |
0.187 |
0.57 |
0.12-2.69 |
0.47 |
Our study illustrated the variability of blood glucose during HD sessions, with a clear downward trend with the progression of HD. This finding was applicable for both patients with and without DM. No statistically significant association was found between the age, duration of HD, or the last meal or snack before HD and the development of hypoglycemia during HD [11-13].
Our study included diabetic and non-diabetic patients and studied blood sugar variability in the immediate peri-dialysis period. In comparison to previously published studies, we found that our results are concordant with Burmeister et al. group who studied the same glucose pattern but included only patients with DM [14]. They, along with other studies [15] also found that the amount of glucose reduction was greater with glucose-free dialysate than glucose-containing solutions. In another study that included patients with and without DM, the glucose fluctuation was found to be higher in patients with DM than patients without it. There was a 2.51 mmol/L reduction of blood sugar level in patients with DM and a 0.75 mmol/L in the non-diabetic patients [7]. In our study, the mean blood glucose reduction was 2.04 mmol/dl, and most of our study patients were non-diabetic patients. The decline in blood glucose during HD could be a result of increased blood volume during HD. Furthermore, HD patients are usually elderly, with malnutrition, impaired renal gluconeogenesis, and reduced insulin clearance [16].
In our study, although some patients experienced hypoglycemia, most of the patients were asymptomatic except for one who had minimal symptoms. We noticed that most hypoglycemia episodes occurred at the last phase of HD [17, 18]. This finding is similar to Sudha et al. [10] study, showing that the significant decrease in blood glucose levels has been mainly occurring at the post-dialysis period. Our study did not observe an association between the patients' age or duration of HD or time from the last meal or snack and the establishment of hypoglycemia during HD. Other studies found that hypoglycemia was mostly related to pre-dialysis blood sugar, especially if it was below 7.7 mmol/dl [14]. Interestingly, all patients who had hypoglycemia in our study had a pre-dialysis blood sugar below 7.9 mmol/dl. Another study suggested the safe cut-off level of 5.6 mmol/dl, especially if the patient is on antihyperglycemic medications [19].
The other risk factor for intra-dialytic hypoglycemia that was studied was dialyzing with non-glucose containing dialysate solutions [19, 20]. In our study, all the patients were dialyzed with glucose-free solutions, which might explain the slightly higher risk of hypoglycemia in our study when compared to other studies, considering that most of our patients were without DM7 [21].
Blood sugar control can be challenging in HD patients with DM. In this fragile group, the physician has to balance between increased risk of hypoglycemia, malnutrition, and the shortlist of proper antihyperglycemic medications that can be used for blood sugar control. Plus, the wide fluctuation in blood glucose between the dialysis day and the non-dialysis days and during each HD session [22].
Apart from the cardiac adverse effects of hypoglycemia, the prompt recovery from hypoglycemic episodes and glucose variations has been related to increased risk of cardiovascular events in patients with DM [23, 24].
Our study had the following limitations; the dialysate used in our research was glucose-free only, so the results cannot be applied to all types of HD solutions. Also, since most of the patients were without DM, we acknowledge that the results might differ between both groups.
CONCLUSION
Our study revealed a clear reduction in the mean blood sugar level during the course of HD sessions. The mean difference in the blood glucose levels between the pre-dialysis and post-dialysis levels is 2.04 mmol/dl were found in diabetic and non-diabetic patients.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None