International Journal of Pharmaceutical and Phytopharmacological Research
ISSN (Print): 2250-1029
ISSN (Online): 2249-6084
Stroke is the third major cause of death worldwide and is a major public health challenge in society. 15 million people suffer from it each year, and one-third is left permanently disabled one-third die worldwide. The average age of onset is above 55 years in western studies which were also found similar in the Indian population. There is a male predominance ratio of approximately 5:1. This study was conducted in Neurology Department at New Government General Hospital, Vijayawada.165 patients were selected out of 152 were selected with the positive response of males and females of the Neurology department. The majority of patients were affected with lower limb weakness 106. Majority of patients were consuming alcohol were 105, [male-104, female-1], followed by smoking 97, [males-87, females-10]. The majority of patients had hypertension as a major risk factor 111, diabetes 92, Hyperlipidemia 90, seizures 66 patients. CT showed clots were in majority 127 than those who had haemorrhage 25. The majority of drugs given to stroke patients are antiplatelets, antihypertensives, Dyslipidemics and antibiotics were. Aspirin was the majorly used drug in a maximum number of 138, followed by Atorvastatin 131, Clopidogrel 113, Citicoline 119. Assessment done by Glasgow Coma Scale had the majority of patients were with moderate scoring 79 [males-60, females-19]. Assessment Done by NIHSS Scale had the majority of patients were under the moderate-severe category 79 [males-63, females-16]. .
INTRODUCTION
According to World Health Organization, stroke is defined as a group of disorders of brain and blood vessels that develops rapidly with the clinical signs and the disturbances of the cerebral function lasting for 24 hours or longer leading to death, which occurs with a vascular origin [1]. Out of these 5 million people die and another 5 million are permanently disabled. High blood pressure contributes to more than 12.7 million stroke cases were reported worldwide. Europe averages approximately 650,000 stroke deaths each year. In the US the prevalence of stroke is about 7 million. The majority of people are over the age of 50-65 years and high blood pressure contributed as the major risk factor. China has the highest rate of deaths due to stroke along with South America and Africa. In India the adjusted prevalence rate of stroke ranges,84-262/100,000 in rural and 334-424/100,000 in urban areas. The incidence rate is 119-145/100,000 based on the recent population studies [2]. Stroke is an acute focal neurological deficit that develops within 24 hours. Thereisischemic stroke (88%), hemorrhagic stroke (12%), and transient ischemic attack. Cerebrovascular accident (or) Stroke is an injury caused to the brain due to poor blood flow which leads to death if not diagnosed in its early stages. It occurs due to the following reasons, the brain cannot receive the needed blood supply due to interruption of blood flow, and rupturing of blood vessels occurs due to invading of blood supply to surrounding areas. Lack of blood supply to a part of the brain leads to hypoxia which in turn leads to brain damage; it is the third major cause of death worldwide and is a major public health challenge in society [3]. Major risk factors related to stroke in the Indian population are the history of hypertension, diabetes, smoking, obesity [4-6]. The modifiable risk factors that contributed to stroke in India are demographic, socioeconomic, and lifestyle. The non-modifiable risk factors for the occurrence of stroke are sex, age, ethnicity, race, genetic factors, and low birth weight. In India diabetes, hypertension, heart disease, smoking, and long-term alcohol consumption are major risk factors of stroke. The choice or decision of drug therapy given is based on the patient's condition. The prescribing pattern and treatment therapy mainly involves drugs like anticoagulants, thrombolytics, angiotensin receptor blockers, antihypertensives, diuretics, statins, cerebral activators, and antiplatelet drugs [7, 8]. A particular dosage and route of administration should be selected according to the patient condition to have optimal therapeutic effects. Primary prevention of cerebrovascular accidents or stroke includes drugs like antiplatelets and maintenance of blood pressure. Secondary prevention therapy includes cardiac angioplasty, carotid endarterectomy, and drugs like warfarin and heparin are useful [9]. A utilization pattern of drugs plays a major key role in the selection of appropriate drugs for the patient. It is an analytical descriptive collection, understanding, quantification, and evaluation of the prescribing pattern [10, 11]. In our present study, we collected cases of stroke patients along with their complete details and our study mainly aims at identifying the prevalence of major risk factors in stroke patients and occurrence of stroke in all age groups along with developing a proper drug utilization pattern. Pharmacists play a key role in designing a beneficial prescribing pattern, providing proper pharmaceutical care, identifying and solving drug-related problems to improve the quality of life of the patient [12-14].
MATERIALS AND METHODS
Sources of data
Laboratory reports, medical records of the patient, direct intervention with the patient, past medical history, patient data collection form.
Data collection
The following data were collected for all patients enrolled in this study. Patient demographic details, types of stroke, history of present illness, medication history, treatment plan.
Study site
This study was conducted in Neurology Department at New Government General Hospital, Vijayawada. It is a 500 bedded tertiary care hospital providing health care services.
Study design
It was a Prospective Observational Study.
Sample size
After patient admission, 165 patients were selected out of 152 were selected with positive responses of male and female of the neurology department. The collected data were entered into a Microsoft office excel sheet according to their age, gender, therapeutic category.
Study duration
This study was carried out for 6 months i.e., conducted from September 2019 to February 2020.
Study criteria
Inclusion criteria
Male and female of age 30 years, diagnosed with stroke
Exclusion criteria
Patients who are diagnosed with carcinoma, coma and serious trauma within 14 days, pregnant or lactating women.
Ethical approval
Written informed consent was signed by all study participants. The study approval was taken from the Institutional Ethical Committee (IEC), Siddhartha Medical College, and Government General Hospital, Vijayawada held on 18th August 2019 with Ethical Committee number – IEC/2019/096G/SMC.
Data analysis
All the collected data were analyzed by using questioner and gives a score according to scales, to assess risk factors and treatment outcomes, quality of life concerning the treatment in neurology patients.
Statistical analysis
Analysis was done by using SPSS software
RESULTS AND DISCUSSION
Categorized the patients based on their gender and age. A total of 152 patients who had a confirmatory diagnosis of stroke were taken into our study. All the demographic details of patients were documented. We mainly assessed the risk factors, severity, and prescribing guidelines in patients along with adverse drug reactions and drug interactions that occurred in the patients.
|
|
|
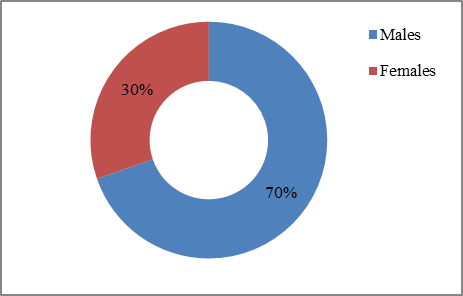
Figure 1. Total Number of Stroke Cases |
A total of 152 (100%) patients out of which 106 (69.7%) patients were males and 46 (30.3%)were female. Males were more prone to stroke when compared to females. The number and percentages were shown.
|
|
|
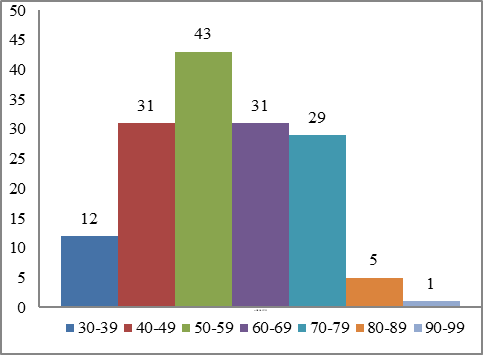
Figure 2. Age Group Categorization of Stroke Patients |
Age group selected for a study of minimum 30 years and maximum 99 years. The patients of age groups between 50-59 years were 43 (28.8%) majority in number and age group between 90-99 years were 1 (0.65%) minimum in number. Stroke generally occurs in elderly people above 45 years and our study also shown that it occurred in elderly people majorly than compared to other age groups.
|
|
|
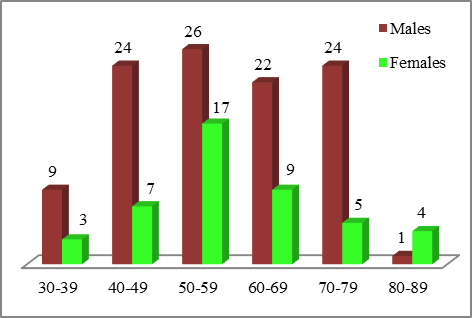
Figure 3. Age Group & Gender Wise Distribution |
Occurrence of stroke was maximum in 50-59 years age group and males were more prone to stroke 26 (24.52%) when compared to females 17 (36.95%) and 90-99 age group showed the minimum occurrence of stroke 1 (0.94%).
|
|
|
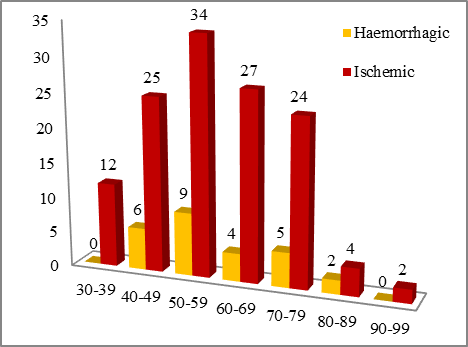
Figure 4. AgeWise and Types of Stroke Distribution |
Cases of both ischemic and haemorrhagic type of stroke in both gender of all age groups. The occurrence of ischemic stroke was observed more in patients when compared with hemorrhagic stroke. The occurrence of ischemic and haemorrhagic stroke was more in the age group between 50-59 years and the minimum in the age group between 90-99 years.
|
|
|
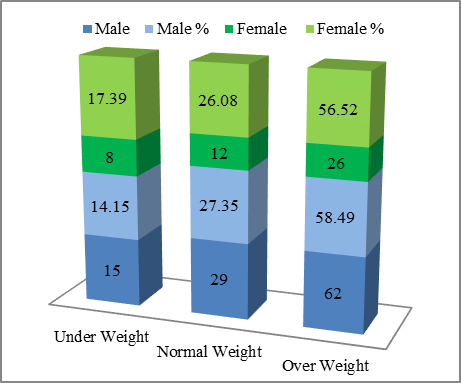
Figure 5. Body Mass Index |
BMI plays a major role in the occurrence of stroke. BMI is divided into underweight, normal weight, and overweight. In our study the majority of patients were overweight 88 (57.89%), (males-62 (58.9%), females-26(56.52%), followed by normal weight 41 (26.96%), (males-29 (27.35%), females-12(26.08%) and underweight 23 (15.12%), (males-15 (14.15%), females-8 (17.39%) were minimum in number.
|
|
|
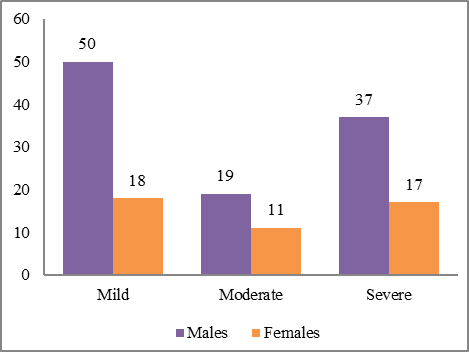
Figure 6. Status of Physical Activity in Stroke Patients |
Physical activity in their daily life of patients was divided into mild, moderate, and severe. Majority of patients were under mild type of physical activity 68 (44.73%) [(males-50(47.16%), females-18(39.13%)], then followed by severe type 54(35.53%) [(males-37(34.90%), females-17(36.95%)], and moderate type had the minimum number of patients 30(19.73%) [(males-19(17.92%), females-11(23.92%)]. A mild and severe type of physical activity is the major reason for stroke. In our study patients with mild type were the majority in number when compared to others.
|
|
|
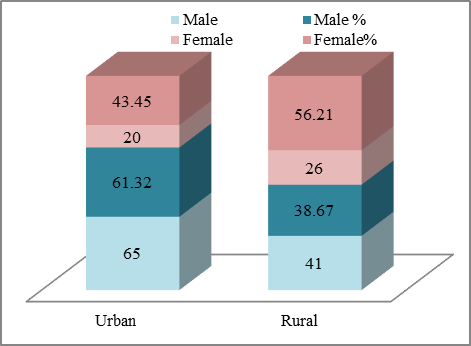
Figure 7. Residence of Stroke Patients |
Patients are divided into two groups urban and rural-based on their residence. Urban residence patients were majority in number 85 (55.91%), [(males-65(61.32%), females-20(43.45%)], when compared to rural residence patients 67(44.09%) [(males-41(38.67%), females-26(56.21%)]. Urban areas are more polluted when compared to rural areas and hence occurrence also is more in people living in urban areas when compared to rural areas. Division based on their residence and gender-wise distribution along with numbers and percentages were represented.
Feeding habits were divided into vegetarian, non-vegetarian and mixed. Majority of patients were with mixed diet 73(48.02%) [(males-50(47.16%), females-23(50.4%)], then followed by vegetarian diet 43(28.28%) [(males-26(24.52%), females-17(39.65%)], then followed by non-vegetarian diet 36(23.68%) [(males-30(28.20%), females-6(13.04%)].
It includesinformation onthe education status of the patients. Majority of patients were uneducated 126(82.89%) [(males-87(82.07%), females-39(84.78%)] followed my educated people 19(17.93%), [(Male-19(17.93%), females-7(15.22%)].
Symptoms like slurring of speech 132 (11.65%) which was observed in the majority of stroke patients, followed by deviation of mouth observed in 116 (10.23%), followed by aphasia observed in 111 (9.79%), followed by altered sensorium observed in 102 (9.02%), followed by left-sided weakness observed in 92 (8.132%), followed by headache observed in 90 (7.94%), followed by tingling sensation 77 (6.79%), facial palsy 76 (6.70%), involuntary movements 66 (5.8%), right-sided weakness 50 (4.41%), chest pain and giddiness 40 (3.53%), shortness of breath 32 (2.89%), ataxia 30 (2.64%), fever 25 (2.20%), loss of consciousness 25 (2.20%), dyskinesia 18 (1.58%), pedal edema 11 (0.97%) observed in a minimum number of patients.
Collected the information about patient’s social habits whether they smoke and consume alcohol. The majority of males were alcoholics and smokers. Majority of patients were consuming alcohol were 105 (69.07%), [(male-104(99.04%), female-1(0.6%)], followed by smoking 97 (63.81%), [(males-87(89.69%), and females-10 (10.30%)]. Smoking categorizations are chain smokers 32 (32.98%), heavy smokers 21 (21.64%), moderate smokers 18 (18.55%), occasional smokers 14 (14.43%), casual smokers 10 (10.30%), recurrent smokers 2 (2.06%).
The major risk factors assessed in stroke patients which showed that majority of patients had hypertension as major risk factor 111 (23.07%), followed by diabetes 92 (19.12%), followed by Hyperlipidemia 90 (18.7%), followed by seizures 66 (13.72%), recurrent stroke 60 (12.47%), coronary artery disease 54 (11.22%), chronic kidney disease 8 (1.666%).Majority of risk factor observed was hypertension [(males-77(20.92%),females-34(20.73%)], diabetes [(male-64(17.39%),females-28(17.07%)], Hyperlipidemia[(males-66(17.93%),females-24(14.63%)], seizures [(males-45(12.22%),females-21(12.80%)],recurrent stroke[(males-40(10.86%),females-20(12.19%)], coronary artery disease [(males-36(9.78%),females-18(10.97%)].Hypertension stages are differentiated according to the gender wise characterisation. normal [(males-8(10.38%),females-1(2.94%)], pre-hypertension[(males-13(16.88%),females-4(11.69%)], stage-1 [(males-19(24.67),females-11(33.35%)], Stage-2[(males-26(33.76%),females-13(38.23%)], hypertension crisis [(males-11(14.28%),females-5(14.70%)].
The diabetic statuses of the patients are prediabetic and diabetic. Prediabetic 56 (60.89%) were the majority in number when compared to diabetic 36 (39.21%). We further divided them according to age-wise distribution prediabetic [(males-29(51.78%),females-19(52.77%)], diabetic [(males-27(48.21%),females-17(47.23%).CT examination revealed bleeds and clots in stroke patients. CT showed that patients who had clots were in majority 127 (83.55%) than those who had bled 25 (16.44%). Patients with ischemic stroke were the majority in number 127 (83.55%), followed by hemmoragic stroke 23 (15.3%), followed by subarachnoid stroke 2 (1.32%). Characterization of the frequency of the type of stroke according to the gender distribution was also done. Ischemic stroke [(males-85(80.18%),females-42(91.30%)], haemorrhagic stroke [(males-19(17.92%),females-4(9.52%)], subarachnoid stroke [(males-2(1.88%),females-0)]
Drug regimens given to stroke patients and observed that antiplatelets, antihypertensives, Dyslipidemics and antibiotics were majority of drugs given to stroke patients. Aspirin was the majorly used drug in maximum number of patients 138(7.61%), followed by Atorvastatin 131 (7.22%), Clopidogrel 113 (7.06%), Citicoline 119 (6.56%).The usage of drug regimens according to gender distribution, Aspirin [(males-100(8.11%),females-38(6.59%)], Atorvastatin [(males-90(7.29%),females-41(7.11%), Clopidogrel [(males-90(7.29%),females-38(6.59%)], Citicoline [(males-83(6.73%),females-36(6.25%)], Ceftriaxone [(males-89(7.21%),females-25(4.34%)]. Characterisation of drug usage regimen based on distribution of type of stroke (ischemic &haemorrhagic) was also done. Aspirin [(Ischemic-127(9.07%), Haemorrhagic-11(3.04%)], Atorvastatin [(Ischemic-108(7.71%), Haemorrhagic-23(6.37%)], Clopidogrel [(Ischemic-120(8.57%), Haemorrhagic-8(2.21%)], Citicoline [(Ischemic-98(7.00), Haemorrhagic-21(5.81%)], Ceftriaxone [(Ischemic-94(6.71%), Haemorrhagic-20(5.54%)]
Characterisation of drugs based on category was also done. Antiplatelets were the majority of used drug regimen 266 (16.77%), followed by Antihypertensives 252 (15.88%), Dyslipidemics 131 (8.25%), Antidiabetic 127 (8.00), Multivitamins 123 (7.75%),Neurotonics 119 (7.50%), Antihypertensive medications used, ACE Inhibitors 93 (36.90%), Alpha+Beta blockers 56 (22.22%), Calcium channel blockers 43 (17.06%), Beta blockers 35 (13.88%), Diuretics 25 (9.92%).Drugs in the Antidiabetic classification into Metformin 60 (46.87%), Glimepiride 40 (31.25%) and Plain insulin 28 (21.87%).Drugs included inthe Multivitamin classification are Calcium+VitaminD3 68 (55.28%), Methylcobalamin 39 (31.73%), Complex 16 (13.01%).To assess the level of consciousness in a brain stroke patient we assessed the scoring by Glasgow Coma Scale. We divided into mild, moderate, severe according to the severity of the patient. Majority of patients were with moderate scoring 79 (51.97) [(males-60(56.60%), females-19(24.05%)], followed by mild 40 (26.31%) [(males-25(23.58%), females-15(37.15%)], severe 33 (21.71%) [(males-21 (19.8%), females-12(36.36%)]. To measure the stroke related neurological deficits in stroke patients we used a quantitative assessment tool called as NIHSS scale. We classify patients into mild, moderate, moderate-severe, severe categories. Majority of patients were under moderate-severe category 79 (51.97%) [(males-63(59.43%),females-16(34.70%)], followed by severe 29 (19.02%) [(males-15(14.15%),females-14(30.43%)], moderate 26 (17.10%) [(males-17 (16.03%),females-9(19.56%)], mild 18(11.84%) [(males-11(10.37%),females-7(15.21%)].
Classification of adverse drug reactions by naranjo’scasuality assessment scale into definite (≥9)-observed in1 patient, probable(5-8) – observed in 2 patients, possible (1-4)-observed in 3 patients, unlikely (≤0)-observed in 2 patients. Epistaxis and headache come under an unlikely type of reaction. Diarrhea, headache, nausea comes under the possible type of reaction. Allergic rhinitis, bleeding from the ear comes under the probable type of reaction. A list of drug interactions can be monitored as given below. Clopidogrel + Aspirin can monitor by calculating bleeding time & clotting time. Frusemide + Aspirin can be monitored by Inflammatory changes in the body. Carvedilol +Aspirin can monitor by checking potassium levels. Frusemide + Metformin can monitor by checking blood glucose levels. Aspirin + Telmisartan can monitor by checking blood pressure levels. Carvedilol + Digoxin can be monitored by checking heart rate & ECG.Frusemide+Pantoprazole can be monitored by checking magnesium levels. Atorvastatin + Aspirin can be monitored by checking serum lipase levels. Furosemide + Aspirin can be monitored by checking liver function tests. Digoxin + Pantoprazole can be monitored by checking magnesium levels. Calcium + Aspirin can be monitored by checking liver function tests.
Statistical analysis
The Prevalence of Stroke among Study Subjects, Prevalence of Stroke (p)=92.12, Prevalence of Ischemic Stroke (p)=76.96, Prevalence of Haemorrhagic Stroke (p)=15.15.
CONCLUSION
In our present study, we concluded that male patients were majorly affected with stroke when compared to female patients due to social habits like smoking and alcohol consumption. Elderly patients of age group 50-59 were majorly affected with stroke. Patients were majorly affected with ischemic stroke when compared to hemorrhagic stroke.
Acknowledgments: We gratefully acknowledge the Doctors of Neurology department of Government General Hospital (GGH), Vijayawada, and Dr. K. Padmalatha, Principal of Vijaya Institute of Pharmaceutical Sciences for Women for support.
Conflict of interest: None
Financial support: None
Ethics statement: Written informed consent was signed by all study participants. The study approval was taken from the Institutional Ethical Committee (IEC), Siddhartha Medical College, and Government General Hospital, Vijayawada held on 18th August 2019 with Ethical Committee number – IEC/2019/096G/SMC.