International Journal of Pharmaceutical and Phytopharmacological Research
ISSN (Print): 2250-1029
ISSN (Online): 2249-6084

Nonsteroidal Anti-inflammatory Drugs (NSAIDs) are the main therapeutic alternatives in treating pain and inflammation among various populations. However, they are linked with some adverse reactions and drug interactions. This review aims to summarize the naproxen mechanism of action and place it in the therapeutic strategy. Naproxen is a reversible inhibitor of the pro-inflammatory enzyme cyclooxygenase (COX) used in clinical practice for control of pain of various origin, namely post-traumatic pain (distortion and sprain), post-operative pains (in traumatology, orthopedics, gynecology, maxillofacial surgery), gynecological pains (pain and discomfort at primary dysmenorrhea, after the introduction of an intrauterine coil, etc.), headache and toothache, prevention or treatment of migraine, spinal pains, extra-articular rheumatism. It has been established that the duration of pain relief after a single dose of naproxen is significantly greater than after the intake of ibuprofen-containing products of equal concentration in the post-operative period of dental intervention. Naproxen is recommended as a drug for the choice of the class of tNSAIDs also in many national therapeutic guidelines (England, Canada, Russia).
INTRODUCTION
Indisputably nonsteroidal anti-inflammatory drugs (NSAIDs) prevail in the prescribed therapeutic approaches constituting approximately 80% of all prescriptions [1-4]. Similar data can be substantiated by the key role of those drugs in pain and inflammation control – symptoms defined yet in ancient times by the Greek philosopher Epicurus as the greatest evil facing humanity [5].
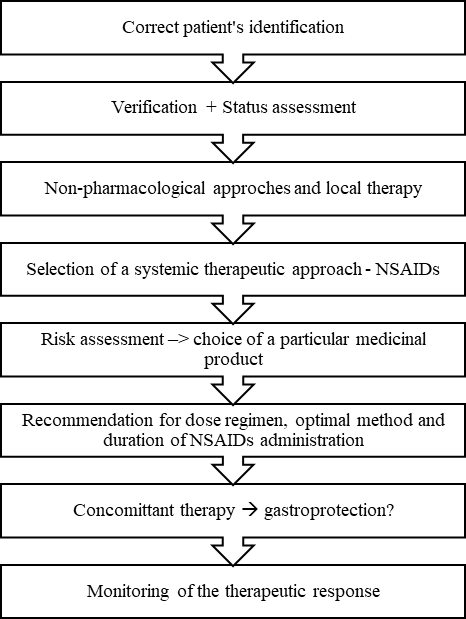
At the same time, the drugs outlined as "deliverance" from febrile conditions, pain syndrome, and rheumatologic complaints are found to be among the leading causes for hospitalization following adverse drug reactions [6-8]. European statistics have reported data for more deaths due to irrational administration of NSAIDs than to road crashes or cancer victims [9, 10]. From the aspect of the permanent trend showing the increasing number of patients needing anti-inflammatory treatment, the adequate choice of an effective and safe nonsteroidal medicinal product is crucial (Figure 1).
In the era of evidence-based medicine, the decision concerning the therapeutic approach is based on two factors – data from randomized clinical trials and/or post-marketing surveys of safety, efficacy, and individual patient characteristics [11-13]. The gold standard in most large-scale randomized clinical trials is one of the oldest representatives of the so-called traditional NSAIDs, namely naproxen. The positive benefit/risk ratio for naproxen has been confirmed also by comprehensive observational surveys and meta-analyses of data supplied by real clinical practice. The evidence for antipyretic, anti-inflammatory, and analgesic effect of naproxen has been accumulated after the impressive nearly 45-year real clinical experience [14].
Safety of nsaids
The increasing NSAIDs administration as well as the poor experience with the VIGOR study and identified cardiovascular risk associated with the implementation of the selective inhibitors of cyclooxygenase-2 (COX-2) [15] shifted the discussion from comparative effectiveness to the safe administration of nonsteroidal analgesics, particularly for patients' groups at risk. The regulators did not delay their reactions – yet in 2014 several additional safety analyses were initiated and the product characteristics of all NSAIDs were obliged to contain a warning concerning the cardiovascular risk associated with their implementation. Thus intensified medicinal vigilance, though, unambiguously confirmed the optimal safety profile of naproxen-containing products. What was more, the most respected drug regulators, including the American Food and Drug Agency (FDA) outlined naproxen as predominantly safe precisely concerning cardiovascular risk [16]. After the established evidence of the large-scale PRECISION trial, the competent authorities re-confirmed naproxen as a standard model for the nonsteroidal anti-inflammatory approach [17]. The reason was that naproxen was a therapeutic approach enabling risk reduction with a view to the low minimal therapeutic dose and long analgesic effect. This is also the cause to dispense naproxen as a medicinal product available over-the-counter (OTC) (ОТС) [7].
|
|
|
Figure 1. Algorithm for the choice of therapeutic approach through NSAIDs |
The analysis of pharmacoepidemiological data for global naproxen use revealed its categorical position as the most frequently prescribed product belonging to the category of so-called traditional NSAIDs (tNSAIDs) (IMS, secondary sales, 2017, EUR, (UK, USA, Canada) [18]. Naproxen is the most preferred anti-inflammatory alternative in countries as the USA, Canada, and the UK with some of the best-organized functioning pharmacovigilance systems and the identification of alerts associated with drug safety is most active [19].
Mechanısm of actıon and therapeutic indications
Naproxen is a reversible inhibitor of the pro-inflammatory enzyme cyclooxygenase (COX). The isoforms COX-1 and COX-2 catalyze the initial steps of transformation of the free arachidonic acid into prostaglandins, involved in nociception, hypothalamic regulation of the body temperature, inflammation, hemostasis, and cardiovascular function. Naproxen mainly suppresses COX-1 activity and to a smaller extent mitigates the role of the enzyme isoform COX-2. In this way, the prostanoid biosynthesis is blocked, especially by the reduced production of prostaglandins G and H [20]. As a result it is applied in clinical practice for control of pain of various origin, namely post-traumatic pain (distortion and sprain), post-operative pains (in traumatology, orthopedics, gynecology, and maxillofacial surgery), gynecological pains (pain and discomfort at primary dysmenorrhea, after the introduction of an intrauterine coil, etc.), headache and toothache, prevention or treatment of migraine, spinal pains, and extra-articular rheumatism. The antipyretic effect enables its implementation in the treatment of infectious diseases as adjuvant therapy to the specific one in addition to its anti-inflammatory and analgesic role. The mechanism of action of naproxen explains also its application for rheumatic diseases such as rheumatoid arthritis, juvenile chronic arthritis, osteoarthritis, and ankylosing spondylitis. For gout patients, the capacity for effective analgesia with the quick triggering of the analgesic effect naproxen is one of the main choice options [21].
Table 1. Indications for Application of Naproxen and Corresponding Optimal Doses
|
Indication |
Standard Therapeutic Dose |
Maximal Daily Dose |
Dose Regimen (Number of Tablets of 275 mg) |
|
Pain Syndrome |
550 - 1100 mg daily |
1 650 mg |
2 - 4 pills |
|
Febrility |
550 mg + 275mg every 6 – 8 hours |
1 650 mg |
2 pills + 1 pill every 6 – 8 hours |
|
Migraine (Prevention) |
1 100 mg |
1 650 mg |
4 pills |
|
Migraine (Therapeutical) |
825 mg + 275-550 mg after 30 min. |
1 650 mg |
3 pills + 1 - 2 pills after 30 min. |
|
Menstrual Pains |
550 mg + 275 mg every 6-8 hours |
1 650 mg |
2 pills + 1 pill every 6-8 hours |
|
Gout |
825 mg + 550 mg after 8 hours +275 mg every 6-8 hours. |
1 650 mg |
3 pills + 2 pills after 8 hours + 275 mg every 6 – 8 hours |
|
Rheumatoid Arthritis |
550 - 1100 mg |
1 650 mg |
2 - 4 pills |
Safety and tolerabılıty of naproxen
Numerous authors support that the various NSAIDs alternatives are similarly effective in pain syndrome control. The optimal therapeutic choice is determined by the safety profile of the particular nonsteroidal analgesic.
There are several factors defining naproxen safety profile:
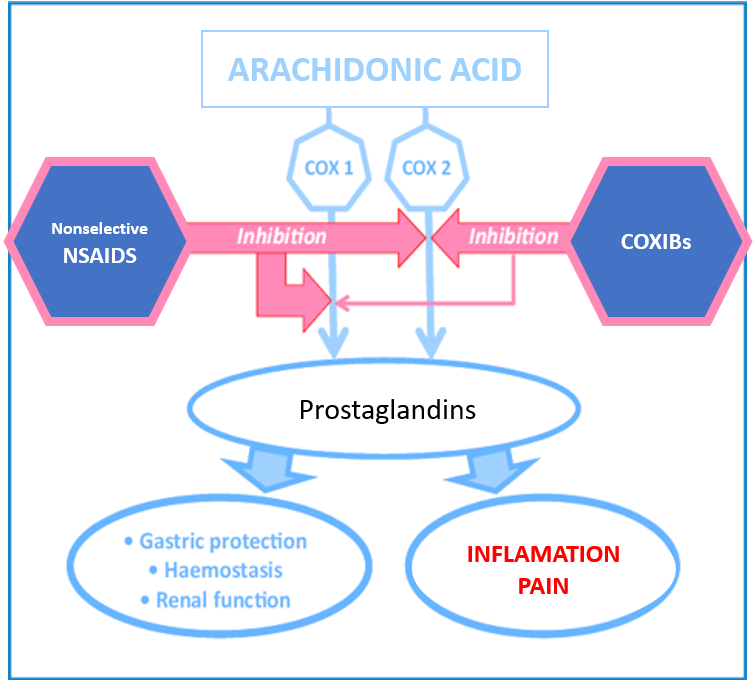
The differential inhibition of the isoenzyme cyclooxygenase (COX) is outlined as the major trigger for NSAIDs cardiovascular safety. The two COX isoforms have a similar structure but a different functional role. COX-1 is involved in supporting the basal prostanoids level, including in the composite synthesis of prostaglandin E2 from the gastrointestinal tract, providing the protection of stomach mucosa against gastric acid and support of the gastrointestinal homeostasis. Besides that, COX-1 catalyzes the production of thromboxane A2 by the activated platelets following a traumatic stimulus. Respectively, the main Adverse Drug Reactions (ADR) associated with tNSAIDs are associated with risk for erosive damage along the gastrointestinal tract but lower risk for cardiovascular incidents as a result of reduced thromboxane A2. On the other pole, COX-2 is responsible for the production of prostanoids involved in the inflammatory response and vasoprotection. The selective NSAIDs inhibit mainly COX-2, in this way reducing the adverse effects on the upper gastrointestinal tract (GIT) mucosa. It is known, though that the higher COX-2 selectivity is associated with significantly greater cardiovascular risk (Figure 2) [22, 23].
|
|
|
Figure 2. The Pharmacological Mechanism of Action of NSAIDs. Adapted from Slim, Karem & Joris, Jean & Beloeil, Helene. (2016). Colonic Anastomoses and Non-steroidal Anti-inflammatory Drugs. Journal of Visceral Surgery. 153. 10.1016/j.jviscsurg.2016.06.011 [24]. |
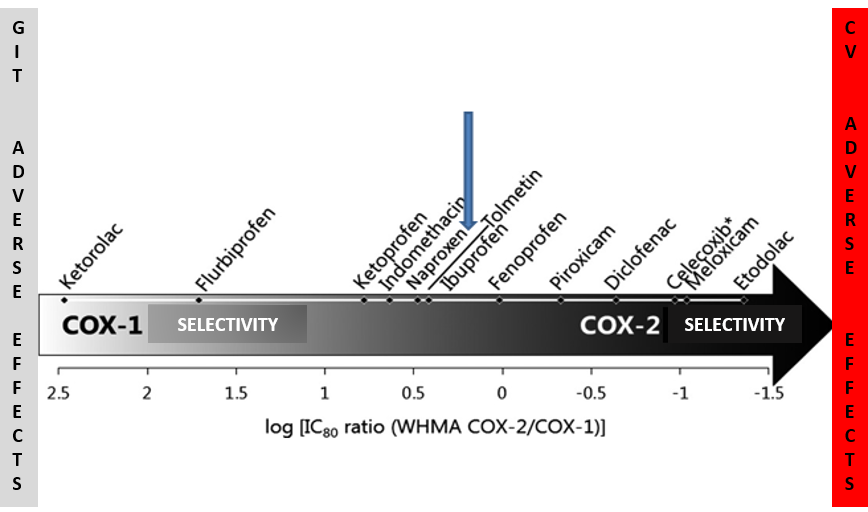
Naproxen is an adequate illustration of how the established low selectivity to the inhibitory potential to the two COX isoforms changes from being a disadvantage into an advantage. Naproxen occupies the "golden mean” referring to observed effects following the selective blocking of COX-1 and COX-2. Many surveys have established that sufficiently effective anti-inflammatory activity was found at blocking approximately 80% of COX-2 potential. Naproxen’s ability to block predominantly COX-1 that is safer for the cardiovascular system and, though to a lower, but sufficient for effective analgesia, the extent to block COX-2 is an elegant approach for effective pain and inflammation reduction at the cost of the easily managed gastrointestinal risk. What is more, many meta-analyses have established that possible naproxen-associated adverse effects on stomach mucosa were better tolerated compared to those of other tNSAIDs (Figure 3) [9, 25].
|
|
|
Figure 3. Relative Selectivity of NSAIDs: COX-1 vs COX-2. Adapted from Danelich IM, Pharmacotherapy. 2015 May;35(5):520-35. doi:10.1002/phar.1584. and based on data from Proc Natl Acad Sci. 1999;96;7563-7568 [25, 26] |
Abbreviations: GIT – Gastrointestinal Tract; CVS – Cardiovascular System; IC80 – Concentration of NSAIDs Necessary to Inhibit 80% of COX Activity; WHMA- William Harvey Human-modified whole Blood Assay
Naproxen's cardiovascular safety is assessed not only based on theoretical postulates derived from naproxen pharmacology. A large-scale study of data from a therapeutic register with more than 83 000 patients with myocardial infarction history found that naproxen application up to 90 days did not elevate the risk for recurrent myocardial infarction or death due to a cardiovascular incident, compared to products containing diclofenac or coxibs [25, 27].
Nevertheless, the cardiovascular safety of NSAIDs is not substantiated only by the selectivity level related to COX-2. The platelet inactivation following the blocked COX-2 as well as the dosing interval and plasma half-life of the particular NSAID have an at least partial effect. The effect of the particular nonsteroidal analgesic on the vascular endothelium and the renal function should not be underestimated as well. That is why it should be kept in mind that naproxen does not cause elevated arterial blood pressure, there is no evidence for clinically significant drug interaction with the chronic intake of low doses of acetylsalicylic acid, and that it has demonstrated better renal tolerance than other representatives of tNSAIDs [22].
The possibility to achieve effective pain relief with lower doses of naproxen due to a satisfactory level of reduction in the inflammation mediators is associated with the balanced COX-blocking potential of naproxen (Table 1).
Pharmacokınetıcs
Naproxen achieves optimal plasma concentration within 2 – 4 hours as a standard when applying a technologically optimal approach for naproxen introduction in the form of a sodium salt. Due to this optimization, the time for achieving maximal plasma concentration is reduced by half. Naproxen sodium salt achieves maximal plasma levels within 1 – 2 hours that combined with the quick action onset – up to 15 min. after the introduction [28] is a prerequisite for quick and effective analgesic effect. Because of this optimized pharmacokinetic profile, naproxen is an optimal therapeutic approach for conditions like headache, dysmenorrhea, and gout where the accelerated start of pain relief is directly determining the individual patient's perception for improvement. Besides, the standard plasma half-life of naproxen is 12 – 17 hours providing long-term effect and the possibility to apply smaller doses at larger intervals. The stable bioavailability of naproxen is one of the strong arguments for its determination as a gold standard in clinical trials of NSAIDs.
Duratıon of effect and dose regımens
The long analgesic effect is important for the effective relief of sharp pain and chronic pain syndrome as well. It has been established that the duration of pain relief after a single dose of naproxen is significantly greater than after the intake of ibuprofen-containing products of equal concentration in the post-operative period of dental intervention. Besides that, a significantly smaller number of participants in the trial who applied naproxen asked for an additional pain-relieving alternative within 24 hours [29]. The administration of NSAIDs with a long half-life, such as naproxen for the treatment of chronic pain has clear advantages, allowing for dosing once or twice daily [30]. The effective analgesia with a smaller number of intakes and quick effect of the applied analgesic are among the foundations of high compliance and adherence to the prescribed administration [30].
Metabolısm
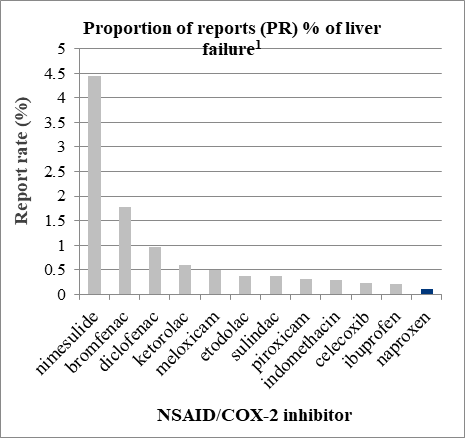
A standard safety concern associated with the administration of all NSAIDs is their effect on liver function and renal homeostasis [31]. Naproxen is submitted to almost full liver metabolism. The considerations for liver tolerance associated with NSAIDs are met by the evidence provided by the system for drug safety surveillance. The statistical evaluation of spontaneous reports for occurring liver failure following the use of NSAIDs unambiguously shows that naproxen has the smallest rate of reported liver failure compared to other popular representatives of tNSAIDs (Figure 4) [32, 33].
|
|
|
Figure 4. Report Rate of Liver ADR as a Result of tNSAIDs. Adapted after Sanchez-Matienzo D et al. Hepatic Disorders in Patients Treated with COX-2 Selective Inhibitors or Nonselective NSAIDs: A Case/Noncase Analysis of Spontaneous Reports. Clinical Therapeutics/Volume 28, Number 8, 2006 [32] |
All NSAIDs can hurt renal function through inhibition of COX1 and/or COX-2 in the kidneys. One of the hypotheses for elevated cardiovascular risk in patients taking NSAIDs is associated with the renal impact and is substantiated with higher blood pressure through COX-2 blocking in the kidneys. Certain studies have found that this effect was observed significantly less frequently, especially if patients use lower doses of OTC products.
Topıcal effects
The local distribution of NSAIDs in the inflamed tissues is of importance for improving the therapeutic effectiveness and reduction of risk for systemic ADR. Naproxen belongs with the so-called “acidic” drugs group (value of acid dissociation constant pKa=4.15) determining the high extent of binding with plasma proteins as well as selective accumulation at the inflammation foci. It is considered that this pharmacokinetic property, at least partially, contributes to the effectiveness and tolerance of naproxen in the treatment of arthritis and gout [34].
Therapeutıc guıdelınes
The National Institute for Health and Care Excellence (NICE) recommends naproxen as a therapeutic approach to the most delicate from a safety point of view population – elderly patients. Naproxen is indicated as a drug for the choice of the class of tNSAIDs also in many national therapeutic guidelines. The pharmacotherapeutic recommendations in countries like Canada, Russia, Slovenia, and England are supported by evidence for effective treating of the pain of various origins and good tolerance, and well managed through gastroprotection of the certain gastrointestinal risk [35-38].
A survey conducted by Levin et al. showed that 93,1 % of the respondents reported a substantial reduction in pain intensity (30% at least) vs. the initial value [39].
Contraındıcatıons
Despite the applied evidence from randomized clinical trials and non-interventional post-marketing studies of the therapeutic effectiveness and safety of naproxen, there is also a set of contraindications for its use. The restrictions for its self-administration do not differ from those common for NSAIDs [7]. The essential groups of patients where naproxen is not recommended are pregnant women, children younger than 12, breastfeeding women, and individuals with diagnosed asthma. Its implementation to patients at antiretroviral therapy is an irrational approach because of the risk for drug interactions; similar is the case of patients with severe heart failure. Naproxen is not sufficiently effective for pains due to endometriosis.
Naproxen and COVID-19?
Despite the statute of “old but gold” standard for nonsteroidal anti-inflammatory therapy, the possible role of naproxen in the fight against the global pandemic from infection with the newly found coronaviral infection is currently actively being investigated. The possible antiviral potential of naproxen against the activity, intracellular invasion, and replication of SARS-Cov-2 has not yet been comprehensively studied. During the last months, in the unclear situation due to the social impatience to discover a cure against the new infection, the hypothesis for non-application of tNSAIDs for COVID-19 emerged [8]. On the contrary, at least the minimally possible option for a positive role of naproxen at COVID-19 infection, as well as the proven antipyretic, analgesic, and anti-inflammatory activities of naproxen are a sufficient argument to include naproxen in the arsenal of symptomatic approaches to relieve the sequences of the coronaviral infection.
CONCLUSION
In conclusion, in the variety of NSAIDs the safety profile of a particular analgesic drug is of yet greater importance for the adequate therapeutic choice. The advantages of naproxen are related to the low minimal effective dose, quick onset of the otherwise long analgesic effect, and the good tolerance on the background of low cardiovascular risk. Those advantages are not only supported by evidence but are also the basic arguments in favor of NSAIDs-treated patients' wellbeing.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None