International Journal of Pharmaceutical and Phytopharmacological Research
ISSN (Print): 2250-1029
ISSN (Online): 2249-6084

The use of Traditional Medicine (TM), has become popular in the world. Despite the benefits, limited knowledge is available especially in the domains of regulation, legislation generally, and specifically homologation. The safety and efficacy of TM have become an important concern for the public health authorities. This study evaluates the knowledge and rates the attitudes and practices regarding homologation of Improved Traditional Medicine (ITM) in Cameroon, specifically in the Mfoundi division.
Our study was carried out with a population of 70 traditional medical practitioners, using a self-administered questionnaire. Interviews were carried out individually with each traditional medical practitioner. At the end, we realized that 61% of the study population expressed knowledge on categories of ITM. According to the TM practitioners with knowledge on the categories of ITM which exist 70% of ITM produced belong to category 2 and 23% belong to category 1. 93% of the study population cited the Ministry of Public Health as the main body in charge of ITM homologation. 51% of the study population declared not knowing the contents of a homologation file, while the remaining 49% had a good level of knowledge on the contents of a homologation file. Only 5% of the population expressed having deposited a request for homologation. In conclusion, we realized that there is a potential in the field of traditional medicine in Cameroon.
INTRODUCTION
For millions of years, men have turned to plants not only for the treatment and prevention of various diseases but also in a bid to improve their quality of life. The use of traditional medicine, as well as complementary and alternative medicine, has become increasingly popular in the world in the past decades. In the world, there has been a renewed interest in traditional and non-conventional medicine [1, 2]. Studies estimate that about four billion people (80% of the world’s population) use traditional and complementary medicine [3].
In developed countries, traditional medicine keeps gaining ground. About 70% of the Canadian population has used traditional medicines at least once. This figure varies for other countries with 31% in Belgium, 42% in the United States of America, 48% in Australia, and 49% in France. According to facts from the fifty-sixth world health assembly of the 31st of March 2003, traditional medicines account for 40% of all health care delivered in China, 40% in Columbia, and 65% in India. About 80% of African and Asian populations use traditional medicines to meet their health care needs [4, 5].
In West and Central Africa, the use of traditional medicine (TM) is very rampant as most (about 80%) of the population depend on these drugs [3, 4]. Cameroon is no exception to this. According to many studies, 80% of Cameroonians use TM [6-8]. The use of TM is also on the rise due to cheaper cost as compared to conventional medicines [9]. Many modern medicines being produced from plants are found in the traditional pharmacopoeia. About 414 medicinal plants from 95 different plant families are used as TM in Cameroon [10-12].
Despite a growing consensus on the benefits of TM, little knowledge is available on it, especially in the domains of regulation, legislation, and homologation. In effect, the safety and efficacy of TM, have become important concerns for the public and health authorities.
According to the World Health Organisation (WHO), only 32% of responding member states reported having a policy on TM/CAM. Of the member states which do not have such policies, 56% report that they are being developed. 28% of member states reported having a national program on TM/CAM, and only 58 member states indicated that they had at least one national institute on TM [13].
National policies on the efficacy, safety, homologation, and regulation of TM are hence the basis for defining the role of TM/CAM in national health care programs, ensuring that the necessary regulatory and legal mechanisms for promoting and creating good practice are made available, and providing equitable access to health care resources.
Homologation is an approbation required nationally as a condition for the marketing of a pharmaceutical product. It can also be defined as the process leading to the acquisition, renewal, extension, or modification (variation) by a pharmaceutical regulation authority, of the marketing authorization of a drug. This process includes the submission of files for homologation request, the study of the file (evaluation), including laboratory control and GMP (Good Manufacturing Practice), and the decision of a competent authority [6].
It is well documented that the use of TM is on the rise across the world. It is also well known that many traditional medical practitioners do not have a clear knowledge about homologation or regulation practices [14, 15]. In low-income countries, the number of practitioners of modern medicine may not be enough to meet needs of the population, hence TM and its practitioners are considered an important part of the health care system, though these they have little knowledge on legislation and homologation. Tradipractitioner is a person recognized in the community in which he lives as being competent to diagnose diseases and other health issues prevailing in that community, and to give health care using spiritual treatments, manual techniques, and/or the use of substances from the plant, animal, or mineral origin [16].
Various TM practices have been developed in many countries and cultures in different regions but without a parallel development of international standards and appropriate methods for evaluating traditional medicine. Sharing national experience, expertise, and information, as well as other useful data, is therefore crucial. If the prevalence of TM use is high and/or the level of awareness on TM, CM, and ITM are found to be significantly poor in our environment, measures on mass sensitization, both to the population and TM practitioners, on what these medicines are, their regulation, homologation, and control will be advocated. If the knowledge on all aspects of TM is found to be low, policymakers and healthcare providers will work on measures to provide quality care to patients, while putting all necessary information at the disposal of TM practitioners in a cost-efficient manner. The general objective was to evaluate the knowledge and to rate the attitudes and practices regarding homologation of ITM in Cameroon, specifically in the Mfoundi Division. The specific objectives of this study were: to analyze knowledge among TM practitioners regarding homologation of ITM, to assess attitudes and practices on ITM homologation among TM practitioners, and to evaluate homologation practices for ITM.
MATERIALS AND METHODS
We carried out a prospective transverse descriptive study in the Mfoundi division of the Centre Region of Cameroon from November and February 2021.
The ethical clearance number N° 135 was obtained from the Ethical Committee of the Faculty and Medicine and Biomedical Sciences of the University of Yaounde I. Participants were recruited in a consecutive non-exhaustive manner. Each participant was interrogated based on a pre-prepared questionnaire. A consent form was filled by the participant before starting any investigation.
To carry out this study, we used a questionnaire designed in four parts: sociodemographic components, knowledge, attitudes and practices regarding homologation of ITM.
Study participants were also given an informed consent form.
We made an inventory of some tradimedical practitioners in the Mfoundi division. They were met in some trade fares, trade medical practitioner’s clinics. After this, appointments were made with them and we carried out interviews.
RESULTS AND DISCUSSION
Knowledge on homologation of ITM within the study population
Definitions
Table 1. Definition of terms
|
Definition |
% |
|
ITM |
91.4% |
|
Homologation |
91.4% |
|
MA |
98.6% |
Table 1 showed that good number of the study population had a good knowledge on definitions of terms with respect to homologation. In effect, 98% of the study population had a good knowledge on the definition of a MA and 91% had a good definition of homologation.
Knowledge on categories of ITM
|
|
|
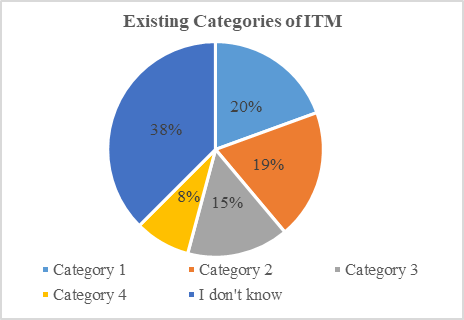
Figure 1. Knowledge on Categories of ITM |
In Figure 1 we noticed that 38% of the study population expressed not having any knowledge on the existing categories of ITM.
Categories of ITM produced among the study population
|
|
|
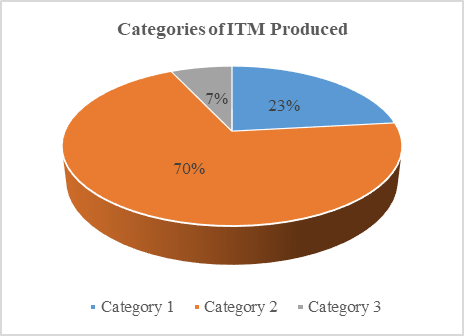
Figure 2. Categories of ITM produced |
Figure 2 showed that 70% of ITM produced belonged to category 2, while 23% belonged to category 1.
Knowledge of homologation procedures
Bodies in charge of ITM homologation
|
|
|
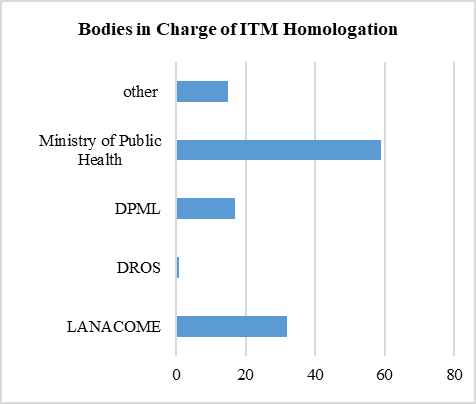
Figure 3. Knowledge on bodies in charge of homologation |
Figure 3 showed that 93% of the population referred to the Ministry of Public Health as the main body in charge of drug homologation in Cameroon.
In fact, DPML means: Direction de la Pharmacie, du Médicament et des Laboratoires/Direction of Pharmacy, Drug and Laboratories; DROS means Division de la Recherche Opérationnelle en Santé/Division of Health Operations Research; LANACOME means Laboratoire National de Contrôle de Qualité de Médicament et d’Expertise/National Drug Quality Control and Valuation Laboratory.
Attitudes towards ITM homologation
Table 2. Attitudes Towards ITM Homologation
|
Variables |
% Yes |
%No |
|
Clarity of information |
68.6% |
31.4% |
|
Accessibility of information |
51.4% |
48.6% |
|
Willingness to get accompanied in homologation process |
92.8% |
7.2% |
In Table 2, 92.8% of the study population expressed their desire to be accompanied in their homologation procedures. 51.4% declared information on homologation was easily accessible.
Practices with respect to ITM homologation
Experience
|
|
|
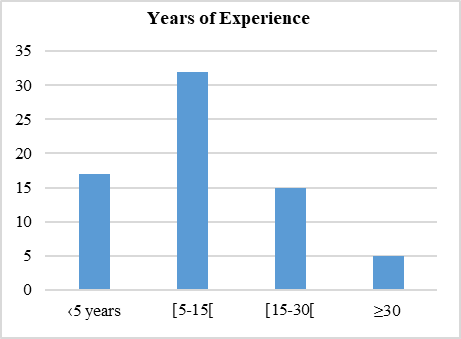
Figure 4. Years of experience of participants |
Figure 4 showed that 45% of participants had between 5 and 15 years of experience practicing traditional medicine.
Homologation
|
|
|
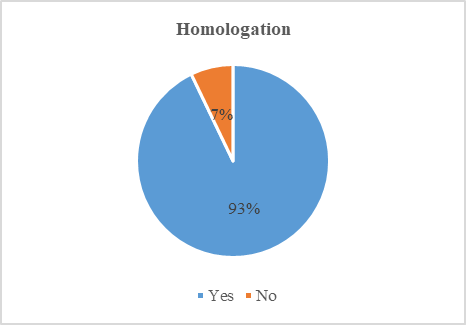
Figure 5. Percentage of study population having proceeded to drug homologation |
Figure 5 showed that 93% of study participants declared never having deposited requests for homologation.
This study was aimed at assessing knowledge, attitudes, and practices regarding the homologation of improved traditional medicines in the Mfoundi division of the Centre Region of Cameroon. This study was carried out to provide high-quality evidence-based data on homologation procedures in Cameroon.
In the course of our study, we faced many difficulties, especially access to tradimedical practitioners.
This was mainly due to a lack of information and lists of tradimedical practitioners of the Mfoundi division. Due to this, we were faced with the inability to increase the sample size.
We also faced challenges getting responses from some tradimedical practitioners we approached, as most of them expressed a lack of interest in participating in the study, while others were not happy with the procedures currently in place.
Knowledge on homologation of ITM
Guidelines on homologation procedures are established, stating that documents need to be deposited at DPML, specifically at the homologation service. Only complete documents are accepted. The documents which constitute these files are either originals or certified copies [21].
Attitudes with respect to homologation procedures
To this effect, the Ministry of Public Health has held meetings with workers in charge of drug homologation to examine homologation files, as well as concertation meetings with the principal actors of traditional medicine [22, 23].
Practices with respect to the homologation of ITM
Only 5% of the population expressed ever having deposited a request for homologation. This was explained, according to the TM practitioners, by the fact that they had limited resources to carry out all tests on the molecules contained in their ITM, to obtain a MA. In effect, ITM containing several plants with many molecules which are difficult to isolate or analyze separately [24].
Also, the development of a new drug based on traditional knowledge and experiences requires the contribution of a large number of stakeholders: traditional healers, ethnologists, botanists, pharmacognosists, phytochemists, chemists, pharmacologists, toxicologists, galenists, and clinicians [25]. Procedures for drug homologation being relatively long and costly, most TM practitioners expressed not being able to meet up all requirements.
CONCLUSION
Our study was aimed at evaluating knowledge, attitudes, and practices with respect to homologation of ITM in the Mfoundi division. We performed interviews with a total of 70 trade medical practitioners, most of whom expressed a great interest in participating in our study. In the course of our study, we realized that there is potential in the field of traditional medicine in Cameroon. Many tradimedical practitioners showed a good level of knowledge on homologation procedures; definitions of terms, categories of traditional medicines, as well as the bodies in charge of homologation in Cameroon.
We realized the tradimedical practitioners showed positive attitudes concerning homologation procedures, as they expressed their willingness to get accompanied in their homologation procedures, as well as enthusiasm to participate in capacitation seminars to improve their vision of homologation in Cameroon.
We also observed good practices with respect to ITM homologation, though a great proportion of our study population had never homologated their ITM before. Nevertheless, there is still a lot of work to be done to reach efficiency and increased inclusion of tradimedical practitioners in the health care system in Cameroon.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: The ethical clearance number N° 135 was obtained from the Ethical Committee of the Faculty and Medicine and Biomedical Sciences of the University of Yaounde I.