International Journal of Pharmaceutical and Phytopharmacological Research
ISSN (Print): 2250-1029
ISSN (Online): 2249-6084
Head and Neck Anthropometric Measurements with Chronic Neck Pain, A Correlational Study
Rajalaxmi. V1*, Jibi Paul2, M. Manoj Abraham3, M. Sasirekha4, D. Naveen Raj5
1,2 Professor, Faculty of Physiotherapy, Dr. M.G.R. Educational & Research Institute University, Chennai, Tamil Nadu, India
3 Principal, KG College of Physiotherapy (Affiliated to The Tamil Nadu Dr. MGR Medical University), Tamilnadu, India
4 Professor, HOD Anatomy, ACS medical college, and hospital, Chennai, Tamil Nadu, India
5 Physiotherapist, TCS, Chennai, Tamil Nadu, India
ABSTRACT
Objectıve: This study aimed to analyze the relationship between anthropometric measures of neck and head with neck pain and its biomechanical variable, dysphagia, respiratory, dysfunction and neck muscle endurance. Background of the Study: Neck pain is the sensation of discomfort in the neck. Neck pain is caused by many different conditions and is sometimes called as cervical pain. In an office, neck disorders that stem from work are problems that are prevalent in workers most especially workers who are always working on computers. Neck pain is a significant public health problem both in terms of personal health and overall wellbeing as well as indirect expenses. Neck pain is prevalent in adults affecting 14-17% of them at some period of their lives. It is a 1-year prevalence in adults ranges from 16 to 75%. The presence of the neck pain tends to vary depending upon the anatomy of the head and neck. This study is done to evaluate the relationship between the anthropometric measures of head and neck along with the neck pain and biomechanical variables. Methodology: A total of 100 samples were selected from 150 volunteers based on inclusion criteria, from the outpatient department in ACS medical college and hospital by purposive sampling method. The purpose of the study was to measure the prevalence of head and neck in relation to chronic neck pain on biomechanical variables dysphagia, respiratory dysfunction, and neck muscle endurance. The questionnaire includes neck disability index questionnaire, swallowing disturbance questionnaire, the peak expiratory flow rate and dials sphygmomanometer for measuring neck muscle endurance were included in the study to determine the neck as well as respiratory dysfunction. Result: From the data analysis, it has been shown that prevalence in male head circumference 21.76±.656, neck column length anterior 5.60±.473, neck column length posterior 5.57±.742, flexion 32.06±4.68, extension 31.56±4.72, right lateral flexion 31.30±4.82, left lateral flexion 31.50±5.36, right side rotation 41.70±10.18, left side rotation 42.50±10.98, neck muscle endurance 35.72±6.01, PEFR 450.50±45.60, NDI 50.80±11.14, SDQ 9.26±2.02. From the data analysis ,it has been shows that prevalence in female head circumference 20.84±.908,neck column length anterior 5.03±.626, neck column length posterior 4.84±.694,flexion 31.80±5.86,extension 31.02±5.15,right lateral flexion 33.00±6.30,left lateral flexion 32.90±5.81,right side rotation 45.70±11.01,left side rotation 45.90±11.01,neck muscle endurance 32.08±3.92,PEFR 4392.40±67.96,NDI 45.40±10.89,SDQ 9.25±2.01. This study result showed changes in the biomechanical variance of both women and men.
Key Words: Anthropometric measures, Neck Biomechanical Variables, Neck Pain, NDI, SDQ, PEFR, Head Circumference, Neck Muscle Endurance, Neck Colum Length, Range of Motion.
INTRODUCTION
Neck pain is very common and is observed that approximately 70% of the people experience cervical pain at any stage of their life [1, 2]. Initially, the problem existed in many professions especially white collared jobs like banking. But with the development of technology and the increased utilization of computers in banks, more health-related problems were created in workers of the banks and other offices. Uncomfortable sitting position and long working hours on computers can cause health-related problems such as fatigue, eye strain and musculoskeletal disorders [3, 4].
Many problems of the structure of head and neck structures such as inflammatory, vascular, degenerative, endocrinal, cancer, and infectious and neoplastic nature Cervical pain can lead to cervical pain [5, 6]. I could also be that cervical pain is caused by zygapophysial joint irritation, disc herniation, and traumatic injuries that may lead to the irritation of the nerves by changes the stimulus. [7]. Neck pain is a common health complaint among adults.[8, 9] Chronic neck pain is reported in up to 22% of women and 16% of men in the general population.[10] The results of a Danish study revealed that out of more than 5000 representative employees, one-third of adult workers of approximately have either moderate or severe neck pain. [11, 12] Risk factors for neck pain share similarities with other musculoskeletal conditions such as genetics, psychopathology (e.g. depression, anxiety, poor coping skills), smoking, sleep disorders, and sedentary lifestyle.[12]
Childs et al report revealed that 10-20% of the population had neck problems, and 54% of individuals have experienced neck pain within the last 6 months. [13] This problem is generally more prevalent in women than in men, higher in high-income countries compared with low- and middle-income countries, higher in urban areas compared with rural areas and peaks at around 45 years of age. The socioeconomic consequences of chronic disorders in the neck and shoulders in terms of early retirement, sick leave, and disability are considerable. [13] Various questionnaires have been designed and developed in recent decades for this aim the neck disability index {NDI}, neck functional disability scale {CDS}.[14-17]
Anthropometry can be defined as the measurement of the dimension and other physical characteristics of the body including masses of the body segments, inertial properties, and volumes center of the gravity. Anthropometrics is the comparative evaluation of the properties and measurements of the human body. Ergonomics is the science of making the workers’ work environment more convenient and safer using anthropometric data and design. There are 2 types of body measurement dynamic and static. Static dimension is a measurement that is sone when the body has a fixed position. Dynamic dimensions are taken under conditions in which the body is engaged in some physical activity.
The neck is an important structure that supports the head weight providing more mobility to the cervical spine on the contrary to stability. Because of this the neck gets commonly stressed leading to neck pain. It usually involves muscle spasm, strain, and tightness of the neck muscles. The presence of problems on the muscle and bones causes limitation of joint range. Neck pain is the sensation of discomfort in the neck area. Neck pain can be due to the disorders of any structures in the neck, including the intervertebral disk and cervical vertebra, Nerves, and blood vessels [18] Neck movement is dictated by the longus capitis, longus colli, and sternocleidomastoid, and for flexion, a concerted effort of the trapezius, suboccopitals, semispinalis, and splenius capitis for extension, and the fibers, sternocleidomastoid, and scalenes from the trapezius to control lateral bending [19]
The peak expiratory flow rate (PEFR), also called peak expiratory flow (PEF), is the maximum expiration speed of a person that is measured with a peak flow meter, which a hand-held and small tool utilized to evaluate an individual's ability to breathe out air. It calculates the airflow through the bronchi and therefore the obstruction degree in the airway. The unit of PEF is usually liters per minute (L/min). The tightness of accessory muscles of respiration and degenerative alterations in the cervical discs cause swallowing difficulties [20]. Reliability The NDI has a fair to moderate test-retest reliability in individuals who have mechanical neck pain and patients with cervical radiculopathy [21] although intraclass correlations can change between 0, 50 and 0,98. These differ
Rence may occur because some studies do not -separate chronic or acute neck pain or due to the fact that the study only used patients with acute neck pain and the retest interval was 72 hours [22]. Validity is tested in different trails by comparing NDI with different instruments: The NDI has good construct validity. [21, 22] Dysphagia is a medical term for the signs of difficulty in swallowing. [23, 24]
Reliability - The intra- and inter-reliability for the CCFT was between “fair to good” and “good to excellent” (ICC: 0.63-0.86). [25-28] Studies of reliability on the CCFT in asymptomatic patiants have determined higher ICC values at the range of 0.81-0.98 [27]. Validity - Construct validity has been proved to be satisfactory [27]. The CCFT discriminative validity is not as strong [27]. One study showed that the CCFT cannot differentiate between those without neck pain, those with a neck pain history but no current pain, and those with current neck pain [25].
METHODOLOGY
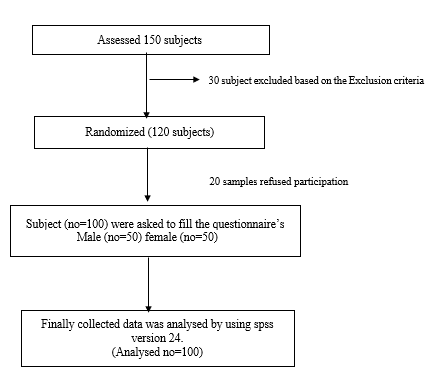
This is an observational study of questioner method. A total of 100 samples were selected from 150 volunteers based on inclusion criteria, from the outpatient department in ACS medical college and hospital by purposive sampling method. The study duration of the study is about 12 weeks conducted from January 2018 to April 2018. The study included the patients who had neck pain for past six months, whose BMI range is between 25-30, the age group of 20-40 years in both genders, whose neck range of motion should be 75% and whose VAS score is between 4 to 7 and based on NDI were included in this study. The patient who had a recent fracture, acute and sub-acute pain, who undergone neck surgery, non-cooperative patient and whose BMI above 30, VAS above 7 and NDI, ROM below 75% were excluded.
Once the study gets approved from IRB ref no IV C- 025, the subjects were fully explained about the study, the questionnaire to be filled and the benefits of participating in the study. The purpose of the study was to measure the prevalence of head and neck in relation to chronic neck pain on biomechanical variables dysphagia, respiratory dysfunction, and neck muscle endurance. Questionnaires were given to 100 subjects and the explanations about each question were given. They were assured of the demographic data confidentiality. The questionnaire given includes neck disability index questionnaire, swallowing disturbance questionnaire, the peak expiratory flow rate, and dials sphygmomanometer for measuring neck muscle endurance were included in the study to determine the neck as well as respiratory dysfunction. Finally, all the data was collected and analyzed.
OUTCOME MEASURE: -
PEFR
Place the pointer at zero and hold the meter in the horizontal position in front of your mouth. Keep your fingers away from the pointer and vents of the meter. Empty your mouth of food or gum to avoid inhaling any foreign substance. Open your mouth and take in a slow deep maximum breath (inhalation). Place your teeth on top of the mouthpiece and close your lips firmly around the mouthpiece so as not to permit any leaks. Forcefully blow out as fast as you can with an explosive force in the shortest possible time. Observe your score and move the pointer back to zero and repeat the measurement in 30 seconds. Select the best reading of two or three efforts and record the results in your diary.
Interpretation of PEFR
PEFR test results are classified as red, green, and yellow zones. Green zone: 80-100 %- this is the perfect zone which shows that your condition is stable. Yellow zone: 50-80% - airway may start to narrow. Red zone: <50% - airways are severely narrowing. Take your rescue medications and contact emergency service.
NDI
NDI is a neck disability index the condition of a specific functional status questionnaire with 10 items including concentration, headaches, reading, lifting, personal care, pain, and work. NDI score contains 0-4=no disability 6-14 mild disability15-24=moderate disability 25-34=severe disability 35 or over=complete disability.
GONIOMETER
The measurements of the cervical motion range are recognized as a part of the assessment of patients with chronic neck pain. A goniometer is a valid tool for measures cervical flexion, extension, lateral flexion, and rotation.
Dials sphygmomanometer
A blood pressure cuff is inflated to 20mmHg and is put between the table surface and the lordotic curve. The patient while keeping the back of the head stable, does a cranial cervical flexion in a graded fashion in five increments (22, 24, 26, 28, and 30 mmHg). The patient remains in each position for 10s with 10 seconds interval between increments. The cranial cervical flexion is carried out by a head nod in the upper cervical spine. Make sure the patient’s jaw is relaxed so that there is not any sternocleidomastoid, hyoid muscle, or recruitment platysma. When a substitution occurs during the head nod or when the pressure decreases below 20%, the test is ended. The normal response is achieving 26-30mmhg.
Strobe flow Chart
DATA ANALYSIS
The collected data were tabulated and analyzed using descriptive Statistics, Paired t-test, Student t-test, and Regression Analysis. All the parameters were assessed using SPSS software version 24. Descriptive Statistics was adopted to find the Mean, Standard Deviation, Percentage of differences, Significance & Linear Regression analysis was done to find the factors associated with Anthropometric Measurement of Head and Neck in relationship with Neck Pain in male and females.
Table 1: Anthropometrıc Varıables for the Male and Female Subjects
|
Variables |
Male |
Females |
Percentage of differences |
Significance |
|
MEAN |
MEAN |
|||
|
Age |
37.40 ± 10.28 |
33.72 ± 6.70 |
-7.30 ± .052 |
.047** |
|
Height (cms) |
164.28 ± 8.72 |
159.46 ± 6.71 |
1.61 ± 8.02 |
.004** |
|
Weight (kgs) |
77.42 ± 12.38 |
66.32 ± 10.92 |
6.51 ± 15.68 |
.000*** |
|
Body mass index |
31.70 ± 2.98 |
26.11 ± 4.22 |
-.514 ± 11.69 |
.072* |
(*- P > 0.05),(**- P ≤ 0.05), ),(***- P ≤ 0.001)
Table 2: Head Cırcumference & Neck Column Length Varıables for The Male and Female Subjects
|
Variables |
Male |
Females |
Percentage of differences |
Significance |
|
MEAN |
MEAN |
|||
|
HEAD CIRCUMFERENCE |
||||
|
HC |
21.76 ± .656 |
20.84 ± .908 |
.582 ± 1.25 |
.000*** |
|
NECK COLUMN LENGTH |
||||
|
ANTERIOR(CMS) |
5.60 ± .473 |
5.03 ± .626 |
.347 ± .784 |
.000*** |
|
POSTERIOR(CMS) |
5.57 ± .742 |
4.84 ± .694 |
.407 ± 1.03 |
.000*** |
(***- P ≤ 0.001).
Table 3: Cervıcal Range of Motıon Varıables for the Male and Female Subjects
|
Variables |
Male |
Females |
Percentage of differences |
Significance |
|
Mean |
Mean |
|||
|
Flexion |
32.06 ± 4.68 |
31.80 ± 5.86 |
-1.41 ± 1.93 |
.757* |
|
Extension |
31.56 ± 4.72 |
31.02 ± 5.15 |
-.814 ± 1.89 |
.427* |
|
Right lateral flexion |
31.30 ± 4.82 |
33.00 ± 6.30 |
-3.31 ± .085 |
.059* |
|
Left lateral Flexion |
31.50 ± 5.36 |
32.90 ± 5.81 |
-2.83 ± .036 |
.056* |
|
Right side Rotation |
41.70 ± 10.18 |
45.70 ± 11.01 |
-8.47 ± .475 |
.079* |
|
Left side Rotation |
42.50 ± 10.98 |
45.90 ± 11.01 |
-7.72 ± .929 |
.121* |
(*- P > 0.05)
This table shows that there no significant differences in the cervical range of motion between the male and female subjects (*- P > 0.05).
Table 4: Neck Muscle Endurance & Peak Expıratory Flow Rate Varıables for the Male and Female Subjects
|
Variables |
Male |
Females |
Percentage of differences |
Significance |
|
Mean |
Mean |
|||
|
Neck Muscle Endurance |
35.72 ± 6.01 |
32.08 ± 3.92 |
1.60 ± 5.67 |
.000*** |
|
Pefr |
450.50 ± 45.60 |
392.40 ± 67.96 |
38.19 ± 78.00 |
.000*** |
(***- P ≤ 0.001)
Table 5: Neck Dısabılıty Index & Swallowıng Dısturbance Questıonnaıre Score for the Male and Female Subjects
|
Variables |
Male |
Females |
Percentage of differences |
Significance |
|
MEAN |
MEAN |
|||
|
NDI |
50.80 ± 11.14 |
45.40 ± 10.89 |
.688 ± 10.11 |
.026** |
|
SDQ |
9.26 ± 2.02 |
9.25 ± 2.01 |
-0.01 ± 0.01 |
.999* |
(**- P ≤ 0.05), (*- P > 0.05)
Table 6: Linear Regression Analysis of Significant Factors in Predicting Neck Pain in association with Head Circumference and Neck Column Length in male and female subjects
|
Variables |
B |
S.E |
P Value |
Beta |
95% Confidence Interval of Exp (B) |
|
|
Lower |
Upper |
|||||
|
Head Circumference |
-.193 |
.044 |
.000*** |
-.350 |
-.280 |
-.106 |
|
Anterior (NCL) |
-.234 |
.064 |
.000*** |
-.289 |
-.361 |
-.106 |
|
Posterior (NCL) |
-.226 |
.047 |
.000*** |
-.360 |
-.319 |
-.132 |
***P<0.001(Highly Significant)
Linear Regression Analysis shows that there is a highly significant association in Anterior & Posterior Neck Column Length and Head Circumference with R2 =.472for males and R2 = .687for females (P<0.001).(GRAPH-I)
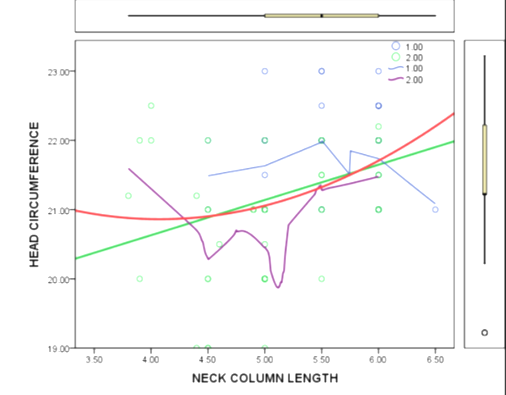
Graph- I: Linear Regression Analysis of Significant Factors in Predicting Neck Pain in association with Head Circumference and Neck Column Length in male and female subjects
1 = MALES, 2 = FEMALES
RESULT
From the data analysis, it has been shown that prevalence in male head circumference 21.76±.656, neck column length anterior 5.60±.473, neck column length posterior 5.57±.742, flexion 32.06±4.68, extension 31.56±4.72, right lateral flexion 31.30±4.82, left lateral flexion 31.50±5.36, right side rotation 41.70±10.18, left side rotation 42.50±10.98, neck muscle endurance 35.72±6.01, PEFR 450.50±45.60, NDI 50.80±11.14, SDQ 9.26±2.02.
From the data analysis, it has been shows that prevalence in female head circumference 20.84±.908,neck column length anterior 5.03±.626, neck column length posterior 4.84±.694, flexion 31.80±5.86, extension 31.02±5.15, right lateral flexion 33.00±6.30, left lateral flexion 32.90±5.81, right side rotation 45.70±11.01, left side rotation 45.90±11.01, neck muscle endurance 32.08±3.92, PEFR 4392.40±67.96, NDI 45.40±10.89, SDQ 9.25±2.01.
Tables 1 & 2 show that there is a statistically significant difference in the Neck Column Length (anterior & posterior) between male and female subjects (***- P ≤ 0.001). Men had significantly higher Neck Column Length (anterior & posterior) than females.
Table 3 shows that there no significant differences in the cervical range of motion between the male and female subjects (*- P > 0.05). Table 4 shows that there is a statistically significant difference in the Peak Expiratory Flow Rate between Male and Female Subjects (***- P ≤ 0.001). Men had significantly higher Peak Expiratory Flow Rate performance than Females. Table 5 shows that there is not any significant difference in the swallowing disturbance questionnaire score between male and female subjects (*- P > 0.05). Table 6 shows that there is a highly significant association in the Anterior & Posterior Neck Column Length and Head Circumference with R2 = .472 for males and R2 = .687 for females (P<0.001).(GRAPH-I) Hence the alternate hypothesis was proved by this study.
This study result showed that both genders changed in their biomechanical variance.
DISCUSSION
In this study with a sample size of 100 subjects with chronic neck pain is included. The results showed a higher prevalence of head circumference, ROM, neck muscle endurance, respiratory problems, and dysphagia. In this present study, it is observed that the subjects with chronic neck pain have lower head circumference decreased range of motion, lower neck muscle endurance and they also have respiratory problems and dysphagia. The prevalence of neck pain is 22-30 % to improve patient functional status and quality of life. In this study, we found that age has a positive correlation with neck pain which is in accordance with the previous studies in neck pain intensity increases as the age increases and the head circumference was higher in male subjects than in female subjects. The correlation between disability and pain was moderate and increases with an increased number of pain sites and factors related to neck pain consequences.
Marchioril and Henderson reported that moderate correlation between pain intensity and neck disability index [27] Harris KD concluded that neck muscle endurance, neck disability questionnaire may be useful measurement to distinguish with different levels of neck pain [28] Michel guez concluded that the overall prevalence of chronic neck pain was higher in females [29].
The endurance exercises were found to be encouraging when compared to the control group; nevertheless, it was considered as a less significant reduction in pain and enhancement in the functional abilities of the neck when compared to the other strengthening exercises group [30]. Motor control exercise has a high impact on neck pain and led to marked relief in pain intensity, disability and in improving the endurance of the neck muscle. Endurance training has also shown a statistically significant improvement, however lesser the significant than the motor control exercise group. In contrast, conventional exercise has found to reduce pain and disability, while there was not any significant improvement in the endurance of the muscle [31]. Endurance exercise is more beneficial in a general exercise program in reducing neck pain and seems to be disadvantageous [32].
Regarding pulmonary function, the findings of this study showed that individuals with chronic neck pain had reduced endurance of their deep neck flexors and reduced range of movement. In terms of neck muscle strength, it was found that their neck extensors were weak, whereas the strength of their neck flexors was not found to be significantly different from the strength of healthy individuals. Patients with chronic neck pain were also found to have a similar forward head posture to healthy controls. Regarding cervical ROM it was found that patients with chronic neck pain have significantly reduced cervical Range of Movement (ROM) in all the planes. The present study also shows that patients with chronic neck pain have a reduction in some of their respiratory flow indices. More specifically, patients with chronic neck pain presented with a significant 6% and 14% reduction in their Peak Expiratory Flow. The study showed that patients with chronic neck pain have decreased pulmonary volumes [26]
CONCLUSION
The study concluded that there is a positive correlation between the neck column length (anterior and posterior) and the head circumference with the neck pain. The study also shows that there is a positive correlation between neck muscle endurance and chronic neck pain. As the study included participants of normal BMI value there is no positive correlation.
The study also concludes that the patient suffering from neck pain of course exhibit swallowing and respiratory dysfunction but not so predominant samples included were said to have neck pain for a maximum of six months.
Authors Contribution
All authors have contributed equally.
Conflict of Interest
'Conflicts of interest: none'
Ethical Considerations
The manuscript is approved by the Institutional Review board of faculty of physiotherapyIRB REF NO: IV C- 025/ PHYSIO/ IRB/2017-2018. All the procedures were performed following the ethical standards of the responsible ethics committee both (Institutional and national) on human experimentation and the Helsinki Declaration of 1964 (as revised in 2008).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients are aware that their names and initials will not be published and an effort will be made to keep their identity hidden, but anonymity cannot be guaranteed.
Funding
Nil, This is a self-funded study
ACKNOWLEDGMENT
I would like to thank the authorities of Dr. MGR Educational and Research Institute, University and the Principal Faculty of Physiotherapy for providing me with facilities required to conduct the study.
REFERENCES


