International Journal of Pharmaceutical and Phytopharmacological Research
ISSN (Print): 2250-1029
ISSN (Online): 2249-6084
|
Evaluation of the Prevalence of C-Shaped Canals in Maxillary Molars by Cone Beam Computed Tomography in Iranian Population
Heshmat Allah Ebrahimi Shahraki1, Vida Maserrat2, Maryam Dalaei Moghadam3*, Amin Tabatabaei4, Fatemeh Forghani5 |
|
1 Assistant Professor, Department of Endodontics, Faculty of Dentistry, Zahedan University of Medical Science, Zahedan, Iran. 2 Assistant Professor of Radiology, Department of Radiology, Faculty of Dentistry, Zahedan University of Medical Science, Zahedan, Iran. 3 Post Grajuated Endodontic Student,Department of Endodontics, Faculty of Dentistry, Zahedan University of Medical Science, Zahedan, Iran. 4 Post Grajuated Endodontic Student,Department of Endodontics, Faculty of Dentistry, Zahedan University of Medical Science, Zahedan, Iran. 5 Department of Endodontics, Faculty of Dentistry, Zahedan University of Medical Science, Zahedan, Iran. |
ABSTRACT
Context: Aims: This study was aimed to assess the prevalence of C-shaped root canals in maxillary molars by analyzing cone-beam computed tomography (CBCT) in Iranian population. Settings and Design: Material and Methods: In this descriptive cross-sectional study, 450 extracted maxillary molars were examined by CBCT (NewTom FP QR-DVT 9000 Verona, Italy) radiography. The images were analyzed using NewToms’ NNT software and examined by an oral and maxillofacial radiologist and an endodontist to determine the absence or presence as well as classification of C-shaped canals. Statistical analysis was done by SPSS version 21.0. Results: Of the 450 teeth studies, 24 (5.33%) had C-shaped canals and 426 (94.66%) had normal anatomy. Moreover, the highest type, observed among the study population, was type B1 (Based on Martin classification). Conclusions: The result of this investigation demonstrated that 5.3% of the Iranian population teeth have C-shaped morphology.
Key Words: C-shaped canal, Maxillary molar, Cone beam tomography.
INTRODUCTION
Accurate cleaning, shaping, and complete filling of the root canal system are the main goals of endodontic therapy [1], which often become complicated due to variations of root canal morphology, especially when the clinician is unfamiliar with these variations, resulting in treatment failure [2]. The pretreatment identification of the morphology of C-shaped canals can facilitate the treatment and prevent irreparable damages to the teeth [3].
Familiarity with anatomical variations and specific characteristics of teeth in different ethnic groups can extremely be helpful by specifying the position of dental canals, which in turn, leads to a successful treatment [4].
C-shaped canal, first reported by Cook and Cox [5] in 1979 is an important anatomical variation. According to some studies, racial background accounts for some variabilities [6-10], commonly observed in Asia, specifically in East Asian countries [11]. There are many studies on the prevalence of mandibular molars [12-16]. Newton and McDonald were first reported C-shaped configuration in maxillary molars in 1984 [17]. In contrast to the C-shaped canals in mandibular second molars, there is only one study about its prevalence in the mandibular first premolar in Iran [2]. Regarding the challenges in the diagnosis and treatment of C-shaped canals, its low prevalence in maxillary molars, and the lack of study about its prevalence in maxillary molars in Iran, this study intended to analyze the prevalence of C-shaped canals in maxillary molars among the Iranian population.
There are different techniques for examining the morphology of C-shaped canals, including staining and clearing, [18] histological examination [19], transmission electron microscopy [20], X-ray imaging, [21] computed tomography [22, 23], and micro-computed tomography [24, 25], among which staining and clearing technique is the most prevalent technique because of its high precision [10]. However, a study reported CBCT as accurate as staining and clearing in the diagnosis of the root canal morphology [3].
This study used CBCT because this technique has overcome the conventional radiography limitations through creating three-dimensional images; thus, CBCT is important for the diagnosis of the root canal system morphology, especially in teeth with complex root canal morphology [26].
SUBJECTS AND METHODS:
The research protocol of this investigation was approved by the Ethics Committee of Zahedan University of Medical Sciences.
The number of samples was estimated at 432 based on a specific formula (n =Z2 ×r/d2), α=0.01, the power of 80%, the prevalence of 6.5% (Martins JN et al., 2016 [27]), and an error rate of 10%, using the Power and Sample Size Calculator. To compensate for a probable sample loss, the samples were increased to 450.
The inclusion criteria were:
No teeth with immature root
No teeth with resorbted canal
No teeth with severe calcification
No teeth with previous endodontic therapy or pulpotomy
A total of 450 extracted maxillary molars, that met the inclusion criteria, were used. The teeth were washed by tap water after extraction and kept in distilled water with thymol iodide crystals until completing the collection. The collection process was conducted by a team of practitioners who understood the aims of the study. After that, the samples were completely washed by tap water and immersed in a sodium hypochlorite solution (5.25%) for 1 hour for disinfecting and removing soft tissues. Then, a scaler was used to remove the calculus and the hard tissue remains on the root surface. The prepared teeth were kept in 10% formalin until used.
CT-Scan
All teeth were scanned with a CBCT scanner (NewTom FP QR-DVT 9000 Verona, Italy) with a thickness of 0.3 mm, 90 kV, and an exposure time of 9 seconds. The tomography sections were displayed in the sagittal, coronal, and axial views, using NewToms’ NNT software. Finally, the images were analyzed by a maxillofacial radiologist and an endodontist according to the agreed definitions for C-shaped canals under the same conditions in terms of space, light, and computer systems. Martin classification [27] was used (Fig 1) in this study. Inter-rater agreement among the radiologist and endodontist evaluators was measured. The intra-rater agreement was analyzed by having the evaluation of one-half of the CBCT images by the radiologist and endodontist in each of the 2 sessions.
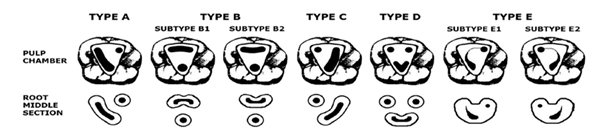
Figure 1: The maxillary C-shaped molar Classification based on the fused root canal position
Data Analysis
The obtained data were analyzed by SPSS (V. 21.0) for the relative frequency and distribution frequency of data using descriptive statistics, tables, and diagrams.
RESULTS:
450 extracted maxillary molars were studied using CBCT for the presence of C-shaped canal morphology. Both of the examiners were consistent in their findings (100% intra-rater and inter-rater agreement).
Out of the 450 extracted teeth, 426 teeth (94.66%) had normal morphology and 24 teeth (33.3%) had a C-shaped morphology. Among 24 teeth with C-shaped morphology, B1 had the highest frequency (25%), followed by B2 and E2 each with a frequency of 16.6%; whereas, D had the lowest frequency (Figure 2). Based on each pair of root fusion, 5 types of C-shaped canals (A, B, C, D, and E) were reported for maxillary molars. (Figure 3)
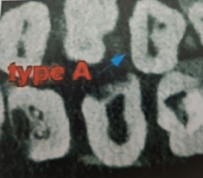
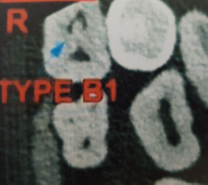
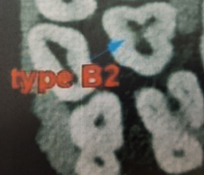
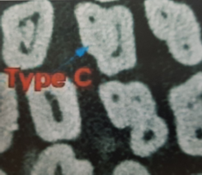
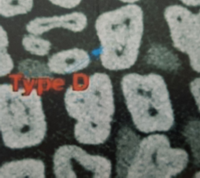

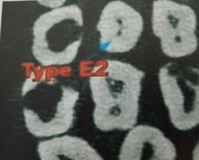
Figure 2. Frequency of various types of C-shaped canals.
Figure 3: Examples of each type of maxillary molar C-shaped configuration (axial sections).
DISCUSSION:
Regarding that there is no specific classification for maxillary molars, this study used the Martin classification [27], which is a modification of the mandibular molars classification. The major difference between the maxillary and mandibular C-shaped molars is in the number of roots. The broader range of C-shaped canals in maxillary molars is because of more combinations of root fusion. Despite the high anatomical complexity, the prevalence of C-shaped maxillary molars is low [28, 29]. The term “C-shaped molar” refers to a large arcuate root canal, which may involve full or partial integration of two or more root canals [27].
The present study was conducted to assess the prevalence of C-shaped canals in maxillary molars in Iranian population by using CBCT and the Martin classification [27]. A total of 450 extracted maxillary molars were analyzed through CBCT, out of which 24 teeth (5.33%) had a C-shaped canal, that D (4.6%) and B1 (25%) had the minimum and maximum frequencies, respectively. In this study, type A was seen in 16.6% of the C-shaped teeth. Type A maxillary molar is characterized by a fusion between palatal and mesiobuccal canals through a deep and large isthmus. Since this isthmus is a suitable place for the accumulation of microorganisms, it can result in endodontic failure if not addressed during the treatment. In type B, buccal canals are mainly stretched from the coronal and medial sections with a semicircular shape towards the oval and circular canal system at the apical end. Types C, D, and E are probably the most challenging types of C-shaped canal in maxillary molars [27].
Various studies have investigated the frequency and prevalence of C-shaped root canal morphology, mostly in the mandibular second molar [8, 12-14], but no study has been done on this subject in Iran. [2]
Martin et al. [27] examined the frequency of C-shaped canals in 2227 maxillary molars in western Europe, among them, 59 teeth (2.6%) were C-shaped with 7 (0.3%) type A, 18 (0.8%) type B1, 10 (0.4%) type B2, 10 (0.4%) type C, one (<0.1%) type D, 5 (0.2%) type E1, and 8 (0.4%) type E2.
The C-shaped canal prevalence was 5.3% in this study and 2.6% in Martin’s study [27] indicating the inconsistency of these studies. We can conclude that the prevalence of C-shaped canals in the maxillary molars is higher in the Central Asian population than the Western European population. This difference can be because of the differences in race, study methodology, and sample size.
Jo et al. [1] investigated the C-shaped canal and root fusion in the maxillary molars of a Korean population through CBCT. Their criterion for the root fusion was based on the Ross classification. They examined 3,553 teeth and reported 63 teeth (1.8%) with C-shaped canal, which was lower than our study. This difference was probably due to the differences in race, methodology, the criterion for C-shaped canal definition, and CBCT software. In the study of Jo HH, type 1, subtype C (MB-DB) was more frequent (n=44, 1.2%), which is similar to our study.
Yang et al. reported a prevalence of 4.9% for the C-shaped canal in maxillary second molar in a Chinese population by using the clearing method [8], which is close to our study [22]. Shalabi et al. [30] found that one out of 83 maxillary first molars in an Irish population had a fusion between the palatal and distobuccal roots, but they provided no additional description about the shape and position of the given canal.
In 2002, De Moor et al. [28] published their 10-year study on 2,175 maxillary first molars through radiographic evaluation in Belgium and reported the prevalence of 0.091% for C-shaped morphology. Their results were inconsistent with ours, which can be due to the differences in race, sample size, and methodology.
Various investigations have proved that C-shaped canals can be diagnosed before the treatment through intra-oral radiography. However, some studies showed that C-shaped canals cannot be easily detected through this method [18]. Therefore, a 3D examination is useful for precise comprehension of the complex anatomical morphology, such as C-shaped canals. Tachibana and Matsumoto [31] used CT for endodontic treatment for the first time. As an obvious advantage, CT allows 3D reconstruction of the root canal system. Recently, CBCT has been commonly used due to lower radiation doses than conventional CT. In fact, CBCT is useful for pretreatment diagnostic evaluation.
Non-invasiveness, high-resolution, low radiation dose and shorter scanning time are other advantages of CBCT over conventional CT [31]. However, conventional radiography has a higher resolution than CBCT. Although conventional radiography is still widely used, it cannot give enough data about the complex morphology of the root canal system. Nevertheless, clinicians should have an acceptable knowledge about the morphology of C-shaped root canals [32].
CONCLUSION
The present study showed that 5.3% of maxillary molars have C-shaped morphology in the Iranian population and CBCT is a suitable and more accurate method for the more accurate evaluation of the root and canal variations.
REFERENCES


